|
Treatment adherence in chronic disease |
|
 |
| Problem |
Why has adherence not improved since the 1970s? Adherence research from the 1970s to 2010s has focused on why people are poor adherers: prevalence, predictors, how to study adherence, how to measure adherence. But if you use the strict definition of intervention study, ie, randomized control trial with both adherence and clinical outcome studied, there have only been 19 intervention studies. Half of them showed a positive effect on adherence.
|
| Overall findings |
Here are the general findings about the state of adherence research:
- Multiple measures of adherence: self-report, practioner report, physiological markers, clinical record review, pill counts, and electronic pill monitors
- Effect sizes: interventions generally have a low-moderate effect size, not becoming greater than 0.37. Multi-focal approaches that incorporate cognitive, behavioral and affective components do better than single focal approaches, probably because of the multiple reasons for non-adherence.
- Predictors of high adherence: self-efficacy, initial adherence, complex regimens, schedule changes or disruptions. However, predictors tend to vary depending on method of assessment
- Non-predictors of high adherence: Demographic factors
- Caveat: People over 75, or "old-old", have worse adherence than the "young-old", ie 60-70 year olds.
- Risk factors: aging neurological system, multiple chronic illnesses, multiple prescriptions, and more side-effects
|
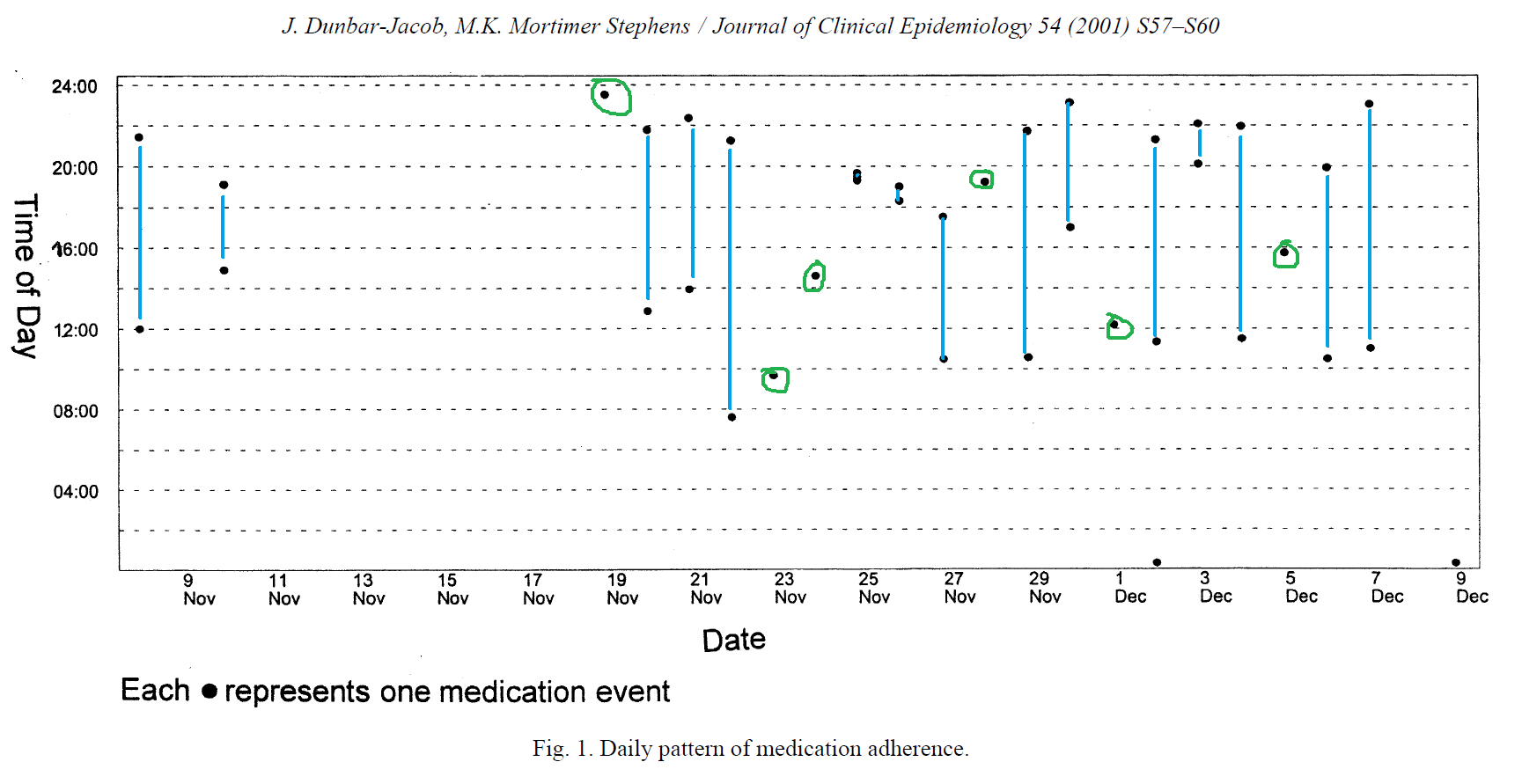
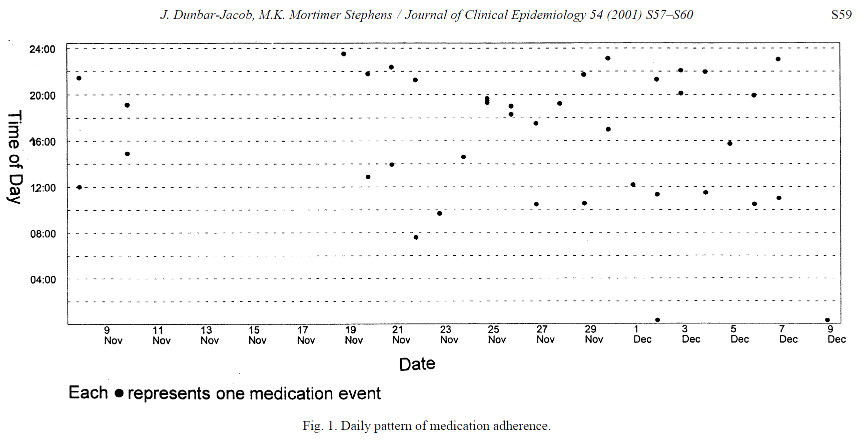
| Variance of adherence |
Here is a picture of the variance in adherence of a twice-daily pill
|
| Recommendations for future research |
- Finding out reasons for missing doses
- Cost-effectiveness of interventions
- Impact on clinical outcomes
- Adherence in chronic disorders
|
|
A meta-analysis of the association between adherence to drug therapy and mortality |
|
 |
| Complaint |
Hey, the effect of adherence should be measured on objective health outcomes, like mortality. Medication adherence is associated with positive health outcomes. There is even association between good adherence to placeboes and mortality. This is called the "healthy adherer" effect, whereby adherence to drug therapy may be a surrogate marker for overall healthy behavior. |
| Main message |
Medication adherence is associated with positive health outcomes in 19 studies of 21 studies. The odds ratio is 0.55 for those with good adherence compared to poor adherence. That means the risk of mortality of good-adherencers is half of that of not-good adherers. Conversely, the risk of mortality was more than double for partipants in drug therapies that proved harmful than poor adherers. |
| Another cool thing |
There is even association between good adherence to placeboes and mortality. This is called the "healthy adherer" effect, whereby adherence to drug therapy may be a surrogate marker for overall healthy behavior. 1997 McDermott found that adherence to the placebo is associated with improved outcomes in 12 studies. DiMatteo found that risk of poor health outcome was 26% lower in good-adherers.
|
| Recommendations to other researchers |
Drug surveillance: stratification by adherence groups could help as good-adherers would have higher rates of adverse drug effects. Usually drug trials will only give an overall average adherence rate.
|
|
Applying User-Centered Design to Movile Application Development |
|
 |
| Main point |
Digia is a Finnish company that makes third-party apps. They made the Nokia Genimap Navigator and the Genimap ImagePlus apps. Here is how they did the usability studies for each of them. |
| Navigator |
They did technology development before the usability experience group came in, so they did not have the chance to do a user needs study. They did a 3-day UI design workshop with the engineers and did paper prototypes. The design was not used completely because they already started implementation. They did a small pilot study with 20 users for 3 weeks, and each person kept a diary. The pilot study found out that the product did not meet their needs. For example, when asking the GPS for "taxi," it would give the administration building of the taxi building. They used this information to revise the UI of the commercial version of the Navigator. Afterwards, they did another usability test and wanted improvements, but it was too late to make it to the delivered product. |
| ImagePlus |
They did a 2-month CD study (whatever that is) with 8 developers. This was a simple image-manipulation app for the phone. They made a long feature list by compiling the editing features of the PC equivalent of editing software. They did a paper prototype and cut down their feature list to save money. To save money again, intead of making a UI prototype, they use actual software implemented for each increment. This is how they found out a joystick was not testing well with users and so they came up with a different method. They used many rounds to get the correct what-you-see-is-what-you-get experience.
|
| Lessons learned |
- Focused CI studues: If you do not have user needs understanding, you can do a CI study (whatever that is) with 6-8 peoeple and analyze the results with affinity diagrams, sequence models and personas.
- Realistic UI prototypes for mobile apps: Constant iterations cost money, cause delays and frustrations. It is best to find usability problems earlier, before implementation.
- Usability testing in the mobile context: Large pilot studies are good, but also really expensive and are typically done too late.
|
| Conclusion |
No feature should be added to the product only because it is easy and cheap to implement, or because you think it is a good idea.
|
|
Early user involvement in the development of information technology-related products for older people |
|
 |
| Main points |
This is about the utopia project.
- The mobile app industry mainly makes apps aimed at the youth market, not older adults
- Older people have significantly different needs, priorities, and expectations than younger people
- The typical developer or researcher will find it easier to design for someone like themselves, and not understand the day-to-day impact of age-related impairments
|
| Older people |
Have to expend more effort into recruiting older adults because they:
- Socially isolated
- Significantly reduced mobility
- Spend much more of their time at home than working people
|
Normal methods of getting data have to be modified.
- Focus groups: they tend to treat this as social hour and get off-topic. One good way to get around this is to make a designated social time, and designated focus group time.
- Self-reporting: cogitive deficits make this inaccurate
- Questionaires:
- They tend to require more certainty before making statements, and will respond "not sure" and will write in "not sure" if that option is not available.
- They also take longer, tire more quickly, and this severely limits the length of sessions.
- They prefer verbally asked questions. This is unrealistic for large projects though
- Spontaneous excursions into the users own experiences, like if the topic were safety alarms, they would show off their own safety alarm
- were often reluctant to critisize products, and asked researchers if they made the app before making a negative comment
- Interviews: The older population is more likely to spend time at home than working people. This group would benefit a lot from home-based technologies, but are also more vulnerable to the negative effects of inappropriate home technologies. This can be mitigated by in-home interviews and observations, and seeing how people obtained their home equipment, how they learned to use it, who supported them, and reporting of good and bad experiences.
|
| Attitudes |
About technology:
- Older people think that they have no use for computers, and are more negative about the amount of effort needed to learn how to use them
- Older people often attribute discomfort to using technology as their own fault rather than failure in design of the technology
|
About UI culture differences between developers and older users:
- Language: widgets, chip, scrolling, original document vs. a copy, monitor, etc.
- They also have a lack of trust in the system and reluctance to experiment. Even experienced older users would stick to a learned sequence of actions, even if that meant taking a huge detour. Speed was less important than "getting the job done."
|
| Conclusion |
Only a third of British companies even think of older people when designing products. There is a lot of work to do.
|
|
How older adults meet complexity: Aging effects on the usability of different mobile phones |
|
 |
| Main point |
Older adults are willing to use modern devices and are interested in modern technology, but they do not think that the devices meet their design and usability needs |
Why?
- hard to implement all the functions in a way that provides good and universal accessibility
- screen size is small
- you cannot see the things in the menu until you open it, and then you have to memorize what is in the menu, create a mental map if it were
- relatively few studies done on older adult requirements for usable mobile phones
|
| Definition |
The definition of usability is "the case with which users interact with the device, achieving optimal performance with respect to effectiveness, efficiency, and users satisfaction." |
| Experiment |
They had 32 people (16 people between 20-30 years, and 16 between 50-65 years) both carry out four tasks on the Nokia 3210 and the Siemens C351. Pretty sure they just asked faculty, staff and students because everyone in the experiment was univeristy educated.
- Call
- Send text message
- Hide own number
- Edit entry in phone book
|
| Methods |
Things measured:
- Time needed to do tasks
- Number of detour steps
- Number of returns to higher levels in the menu
|
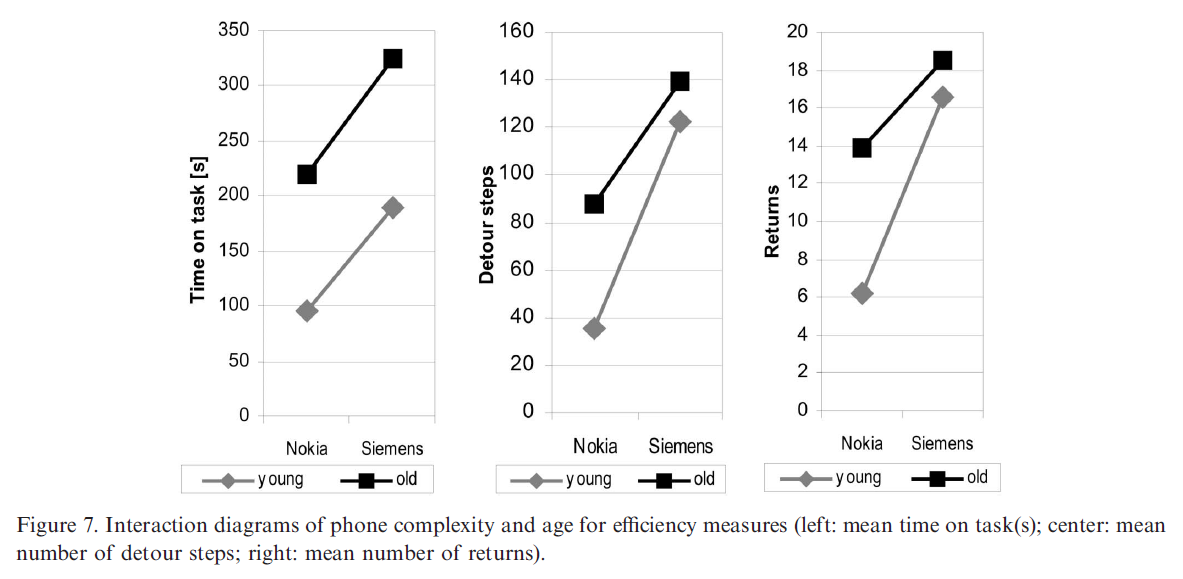
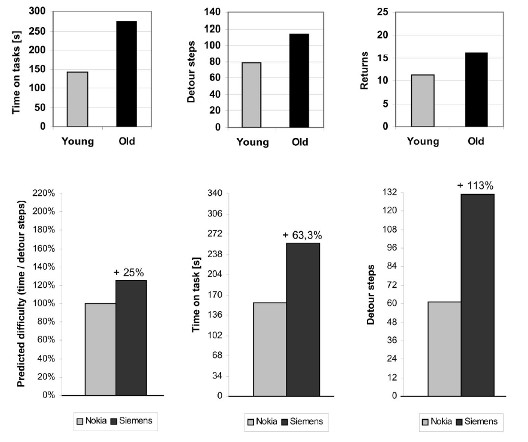
Results:
- Younger users solved 97% of the 4 tasks, whereas only 76% of the older users did
- Younger users spent 2 min 22 sec on each tasks, whereas older users needed 4 min 32 sec
- Younger users did 79 detour steps while older users made 113.6 detour steps
- Younger users went back 11.4 times while older users went back 16.2 times
|
Efficiency measures and cognitive complexity
|
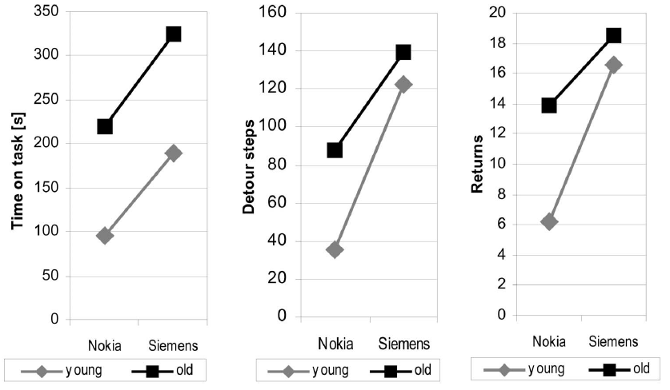
Interaction diagrams of phone complexity and age
|
| Discussion |
Compared to their younger friends, older adults solved 43% fewer tasks, spent 48% more time, took 36% more detour steps, and returned to the top menu 35% more. Older adults said they were less willing to struggle through a jungle of menys, did not want to search for a function, and wanted functions in easy reach with maximum transparency. They preferred the simpler phone. They were also more cautious and reluctant when navigating, and took fewer keystrokes through time. Older adults took longer detours, so if they continued on the wrong path, they would go down it longer. They also had trouble remembering which paths they already took and which ones were new. |
|
"Medication noncompliance: an issue to consider in the drug selection process" |
|
 |
| Main tip |
You should tailor medication regimens to the patients usual daily schedule and lifestyle |
| Things we already know |
An overview of things we already know.
- Bad health arises from non-adherence
- Everyone is non-adherent, even organ transplant recipients
- It costs a lot of money
- Although old people have a disporportionate number of medications, they are not more or less adherent than everyone else
|
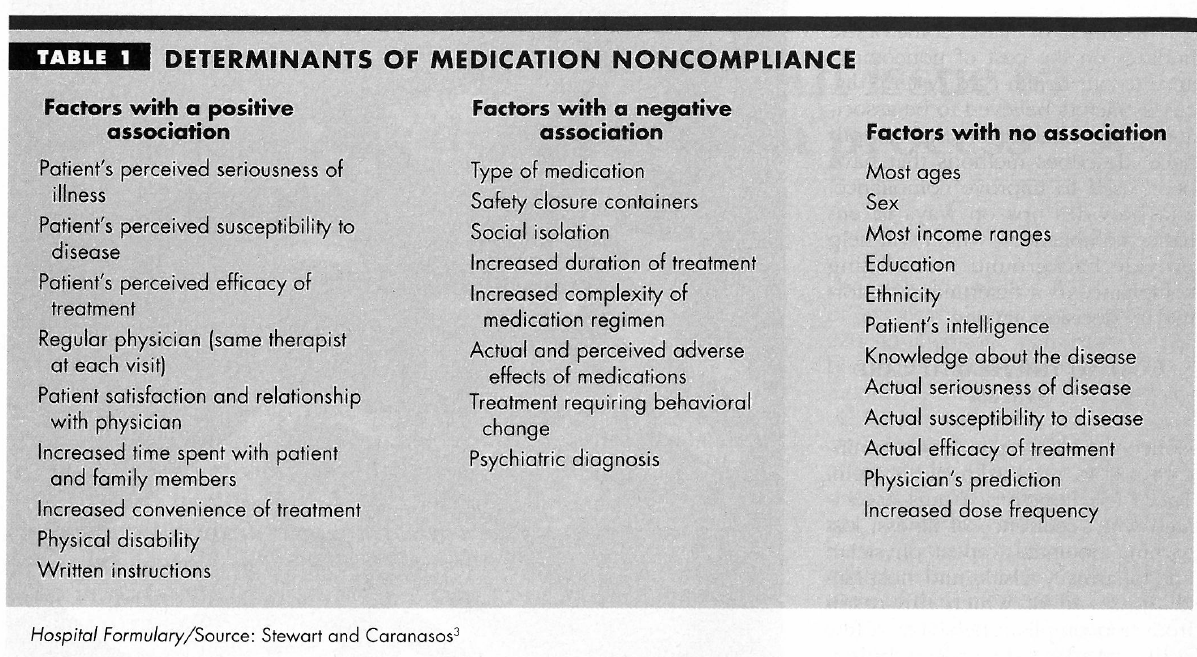
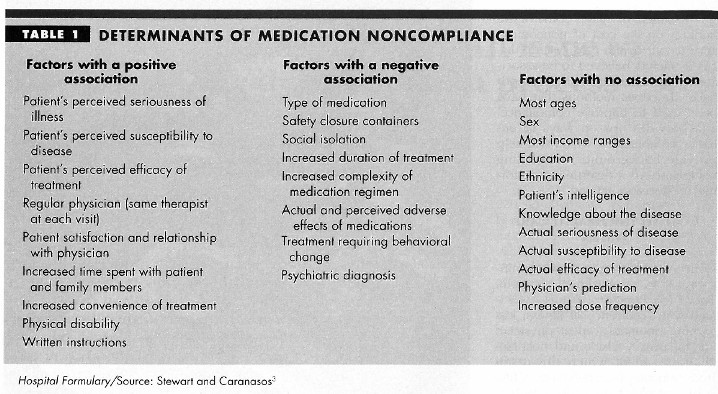
| Mythbusters or not |
Positive predictors of adherence
- Patient perception: percetion of the seriousness and susceptibility of his illness, and the efficacy of his drugs
- Physician-patient relationship: more satisfaction the better
- Therapeutic regimen: the simpler the better
- Disease: Surprisingly, compliance is higher for chronic diseases like antihypertension, diabetes, and asthma than antibiotics. It is also higher for asymptomatic things like analgesics, antacids and sedative-hypnotics than things you take for symptoms
- Family members who spend time with patient
|
Table 1
|
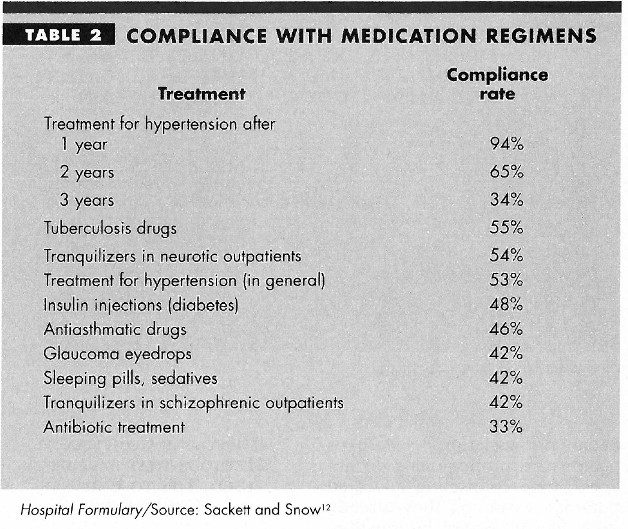
Negative predictors of adherence
- Social isolation
- Child saftey containers
- Treatment requiring behavior change
- Psychiatric diagnosis
|
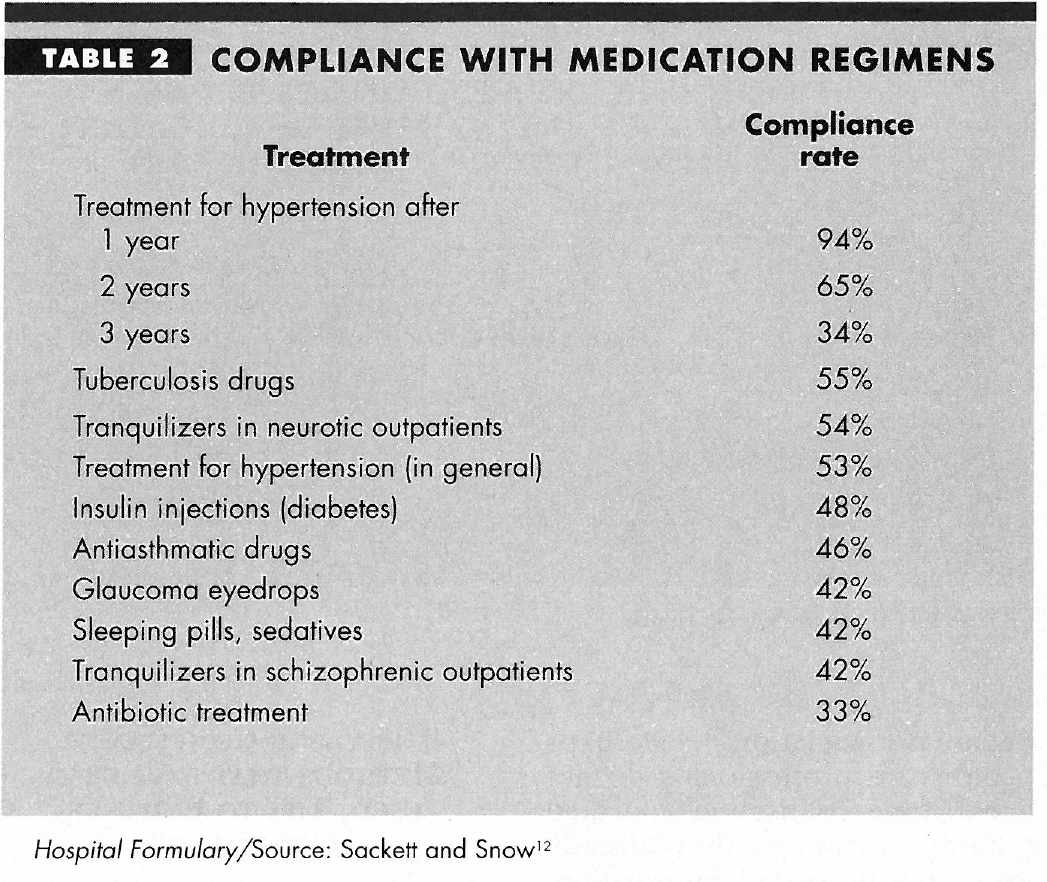
Table 2
|
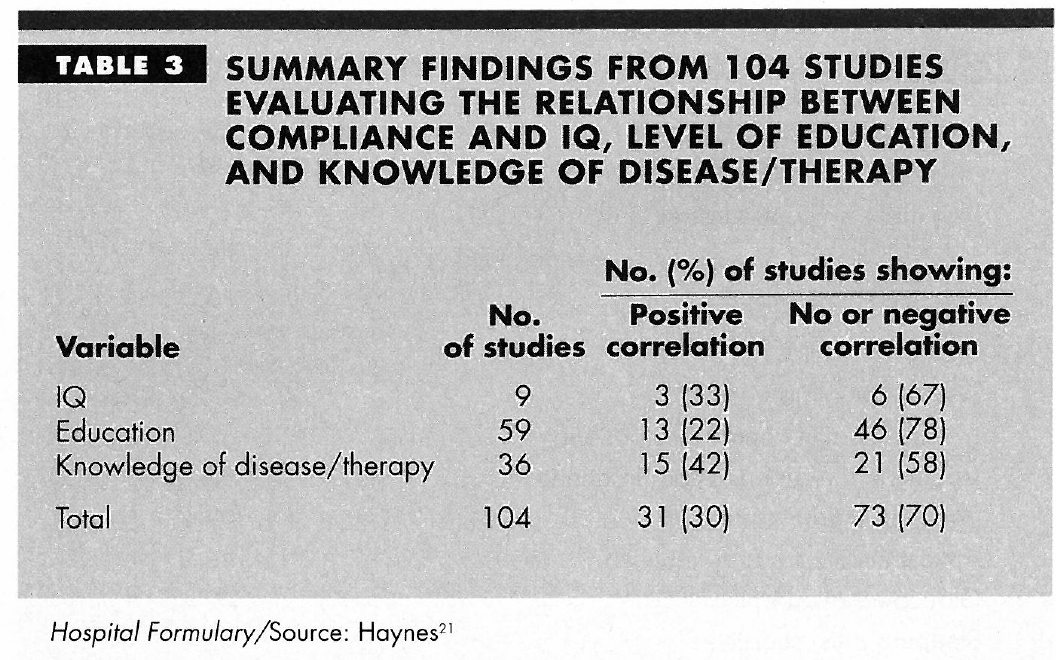
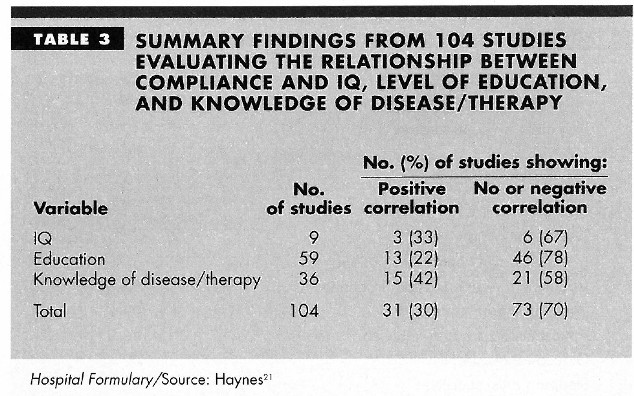
Not predictors of adherence either way
- Age
- Education: surprisingly, there is not. It might be because doctors do not think they need to educate their more educated patients, or the educated ones think they are smarter than their doctors
- Medication cost: this has been a bit more limited but still, doctors should try to prescribe the least expensive option
|
Table 3
|
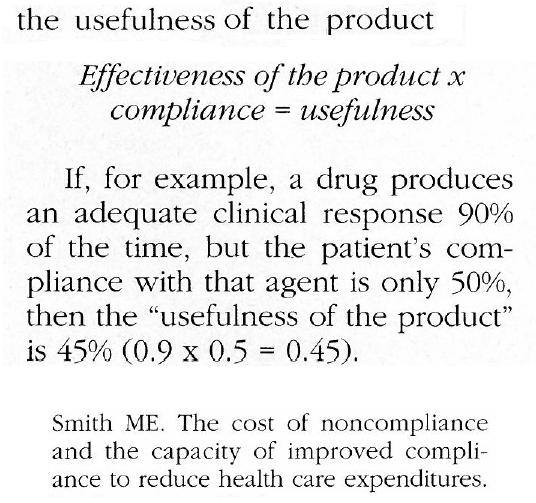
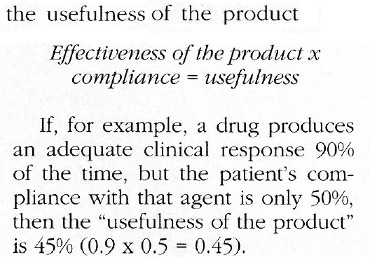
| Usefulness formula |
A suggested equation: the usefulness of a medication, which is effectiveness * compliance = usefulness. |
Usefulness formula made by Smith
 |
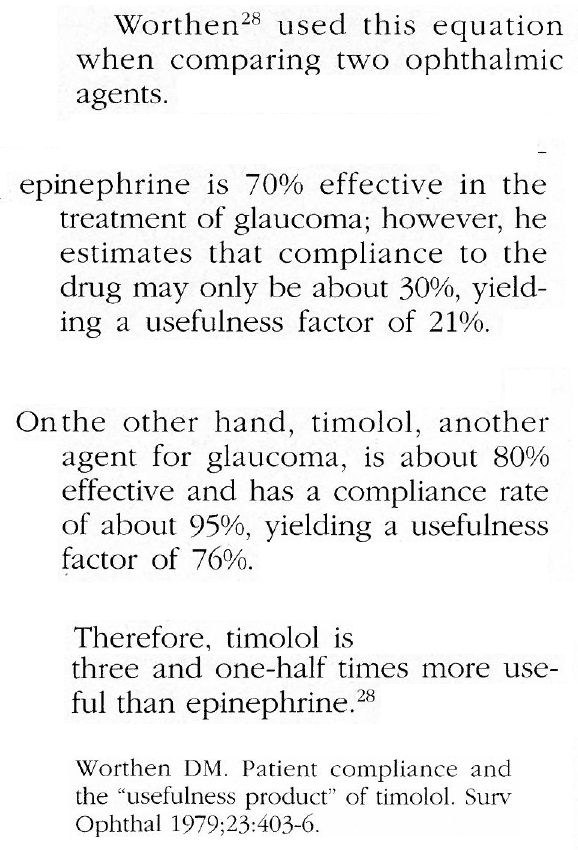
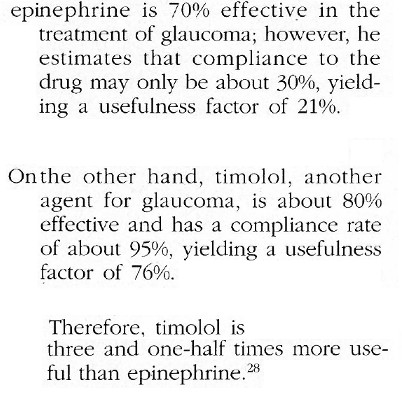
For example, epinehprine and timolol are both things you can take for glaucoma.
Epinephrine has an effectiveness of 70% and timolol has an effectiveness of 80%.
You would think they would be sort of equal, but ephinephrine has a compliance rate of 30%, so it has a usefulness of 21%.
Timolol has a compliance rate of 95%, giving it a usefulness rating of 76%.
This makes it 1.5x more useful than ephinephrine.
|
Usefulness formula applied by Worthen
|
|
"Touchscreen mobile devices and older adults: a usability study" |
|
 |
| Overview |
How do older users feel when using a touchscreen versus a button-based product? |
| Title |
Things to read:
|
| Introduction |
The assumption that older adults wish to avoid using new technology is a misconception:
|
Differences in usage among older people:
|
| Methods |
Semistructured interviews, and then they did a series of tasks on a touchscreen phone and then a button phone. The tasks were:
- Call home from the contact list
- Add a number to the contact list
- Write a text message and then send it
- Set an alarm for 5:30 pm
|
| Recurring themes |
- Nagivating through the menu causes confusion
- Apprehension about their capabilities in interacting with the technologies
- Considered themselves "too old" to be using technologies this advanced
- One participant said he was happy with the phone, as he thoguht it would be much harder. But other people whined so it seems that developers have not really designed it so everyone can use it
|
| Recommendations |
Do more research on older adult user perceptions to make sure that their desires, as well as physical and cognitive needs, are being met |