Current methods of measuring medication adherence are not good enough:
Pill counts - most common, not granular, over-estimate adherence, not granular by time
Surveys or self report - overestimate adherence
Medication Event Monitoring System (MEMs) - not handy if you want to segment your pills
Pillbox requirements
There are four requirements for a portable, multi-compartmental, simple electronic medication tracking device:
Multiple compartments
Portable
Must not require too much interaction for tracking - must be very intuitive
Adherence data must be available at least daily - wireless transmission, real-time data, yet must not drain the battery
Device
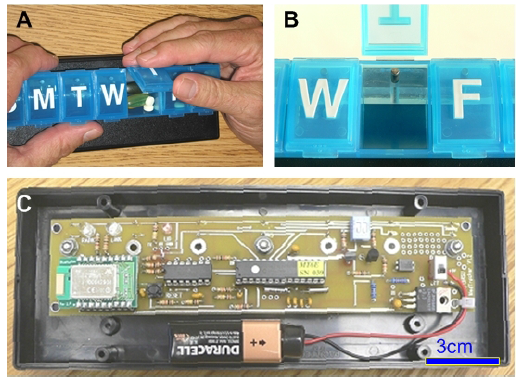
The development of the pillbox was pretty cool. Unlike a heavy "smart" medicine cabinet, they needed a smart portable pillbox that looks and feels like the ones sold at drugstores. It needed to be light and battery operated, so it only sends a wireless signal to a Bluetooth twice a day. They also used a plunger to detect door openings rather than a magnetic strip, because the strip could fall off and then be swallowed.
This is the pillbox, called the Medtracker. B is a closeup of the plunger, which activites a switch that records door openings.
Results
They got 39 elderly people to take a vitamin C tablet twice a day.
Overall adherence was 79%, confirmed by pill counts
Self-reports averaged 93%
12% of subjects believed they never missed a dose, versus 5.3% who actually never did from MedTracker data
The Medtracker also found that pulls were taken from the wrong subcompartment 27 times.
Conclusion
These tracking devices offer much more granular ways of tracking adherence
James Spader likes a cluster-randomized mobile app intervention for diabetes!
This intervention tested a mobile and web-based patient coaching app on diabetes patients.
Results
Groups
Change in glycated hemoglobin %
Control - usual care (UC) - usual care
9.2 to 8.5, down 0.7%
coach-only (CO) - a patient-coaching system includes a mobile diabetes management software and a web portal. Patients can enter data like blood glucose values, carb intake, medications, and other notes. They get automated, real-time educational, motivational, and behavioral messages specific to entered data. The web portal had a messaging center, a personal health record, a library, and a log book. The doctor only got the information if the patient shared it.
9.3 to 7.7, down 1.6%
coach PCP portal (CPP) - Everything in the CO group, but the doctor also had raw, unanalayzed data
9.0 to 7.9, down 1.1%
coach PCP portal with decision support (CPDS) - Everything in the CO group, but the doctor also had analayzed linked to standards of care and guidelines
9.9 to 7.9, down 1.9%
Final
Although they also collected information about diabetes symptoms, distress, and other clinical outcomes like blood pressure and lab values, the only thing that changed was the hemoglobin. Was it a lot? Hmmm, not convinced. Too bad they stratified based on doctor knowledge, and not the individual elements of the intervention.
James Spader likes finding out why reading pill labels are is so hard!
Improving prescription drug container label instructions can improve patient safety. Although it is a simple task, there are various sources of failure.
Methods
Structured cognitive interview of 57 patients
4 different pills
"How would you take this medicine?"
Awareness of auxillary or secondary warning labels
"Show me how many pills you would take" *gives patient a pile of candy pills*
Reponses were analysed using grounded theory. Grounded theory is a systematic method for generating theoretical statements from case studies. It guides the inductie process of organizing content derived from patient responses.
Recommendations
Explicitly describe dose intervals: "Take one pill in the morning, and one pill the evening" instead of "twice daily"
Organize label to minimize distractions: pharmacy logo, doctor name, drug serial number should not take up too much space
Simplify language - use numbers rather than text equivalent, no jargon or awkward terms
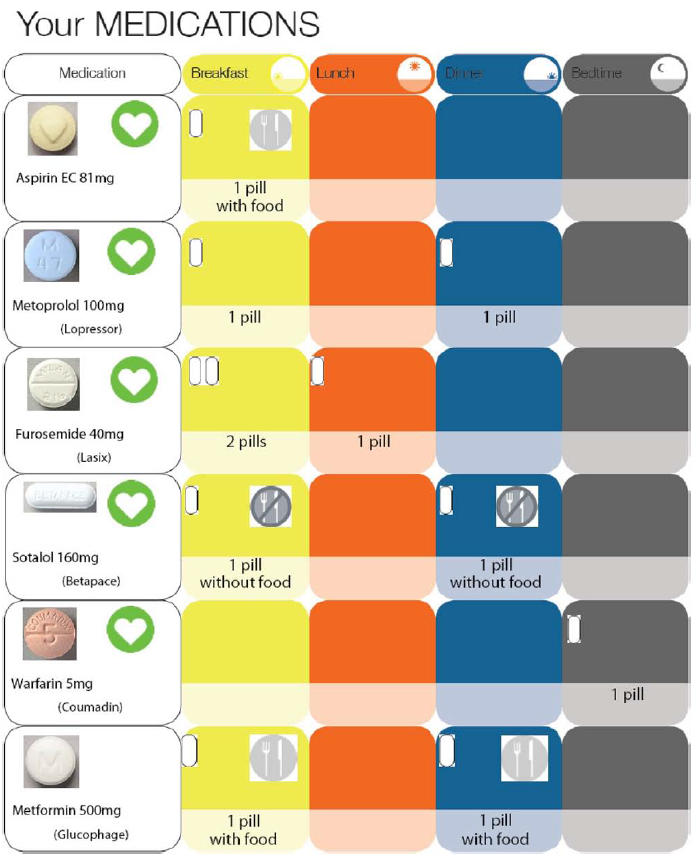
James Spader likes an illustrated paper pill card!
Pictorals are useful for conveying drug indication, dosing schedule, special instructions for administration, side effects, and the importance for completing the full course of therapy.
Self efficacy is a key construct of social cognitive theory is the your judgement of your ability to execute an action or perform a skill. In this paper, they used a new measure of self-efficacy called the Self-Efficacy for Appropriate Medication Use Scale (SEAMS). Cognitive impairment was tested with the Folstein Mini-Mental State Examination (MMSE).
Results
Every 3 months, the pill card was updated against the current medication list in the pharmacy.
Here are the main results:
People liked it: 40% of participants used it everyday, 25% used it every week
They kept using it: 73% of participants who first used it continued to use it at follow-up 3 months later
They showed their doctor: 25% of participants showed it to their doctor
Self-efficacy not increased by pill card use, nor was self-efficacy co-related to any behavior
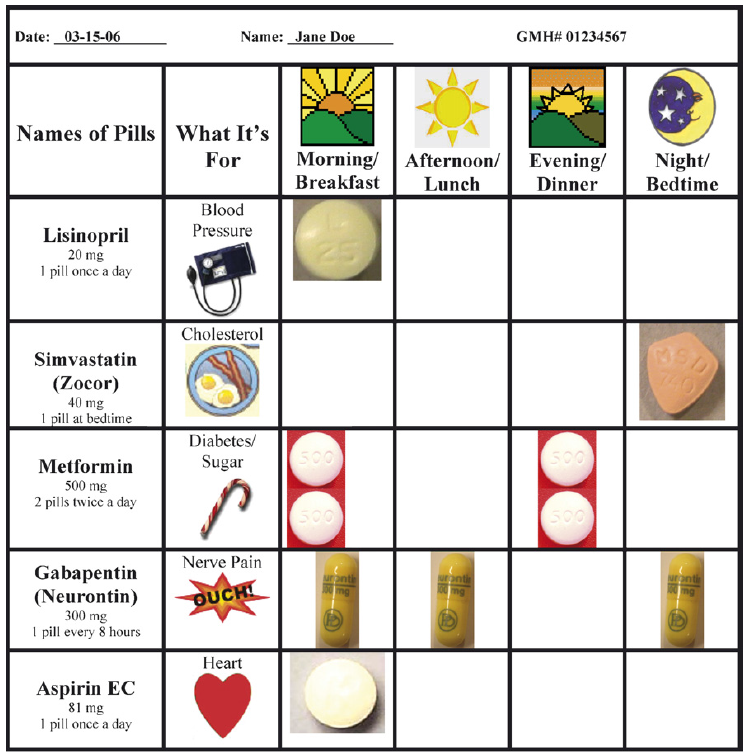
Sample pill card. It has medication names, the purpose of the medication, the time of dosage, and a picture of the pill.
James Spader likes using PDAs to improve adherence!
A typical persuasive system is a stand-alone application used as a tool to detect a potential change in user attitude and/or behavior. However, a Behavior Change Support System (BCSS) is a comprehensive socio-technical platform that provides extended support with a combination of software features and psychological theories. A user can set his own goals and target behaviors using a BCSS. Try using an outcome/change (O/C) matrix to analyze those goals.
Definitions
Outcome/Change
An outcome/change (O/C) matrix can identify goals and persuasive strategies. For example, smoking cession is A/B and forming a behavior is F/B.
Outcome
F-outcome: Formation
A-outcome: Alteration
R-outcome: Reinforcemen
Change
A-change: Attitude change only
B-change: Behavioral change only
C-change: Compliance or conformation, users comply with newly acquired behavior
Interesting notes
Social influence features were rarely found in the evaluated applications. Users can monitor their own progress but they cannot see how their fellow users are doing.
Uniquitous computing focuses on automated capture and access to live experiences. This takes advantage of using the network of caregivers that are involved in the care of older people. They also use persuasive technology to engage patients in taking their pills, not simply reminding. Movipill gives more compliant users more points, and includes a social competition for who can be the most compliant patient.
Persuasive strategies
Counseling strategy - focused on patient education, risk factors for non-compliance. This has mixed efficacy.
Simplified regimen - drug reminders charts, calendar packing, and dosage boxes. However, this strategy alone has not been shown to improve drug compliance.
Compliance aid - this has been shown to be one of hte most effective strategies in improving compliance. These are typically telephone follow-ups by a pharmacist, however, these do not scale well for a large population on a long-term basis. Reminding packages help, but they do not really engage the patient.
Chief complaint
Users will try to take their pills at the right time, otherwise their friends will do better than they do and get more points.
You get happier emoticons the closer to the pre-specificed time you take your pills
The user interface was very simple, with only a Dose screen and a Game screen. In the dose screen, the user can tell the app whether or not he has taken his dose, and the game screen displays the status of the game, including social competition.
The MoviPill interface has a dose sreen on the left, and the list of friends on the right and how often they are taking their pills.
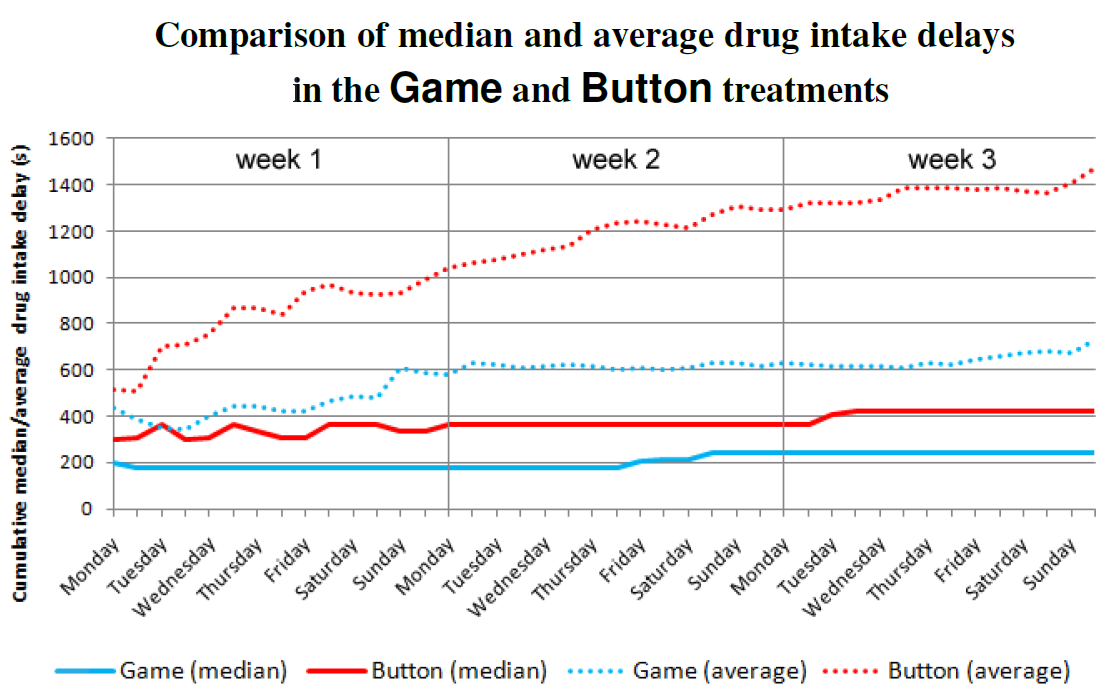
There were two interventions: Button and Game. In the button treatment, participants had to take their own pills but remember when to take it. In the game treatment, there was the same thing, but there was also the game screen in which there was social competition. In addition, an alarm rang 15 minutes after the pill was supposed to be taken.
The median drug intake delay improved 43% when users switched to the game. When you take out the users who said they did not want to play the game, improvement was 56%.
Comments
Here are some interesting results:
The prescribed intake time did not correlate with medication compliance
Users who really wanted to win the game and pressed the button a lot were more likely to enjoy the game
Reminders had no affect on medication compliance
Different rewards for different users: getting a game points reward was ranked last in a list of 4 potential prizes, the other three being money, discounts on their phone bill or store, or a picture from their grandchildren. When the people who ranked the game points last were taken out of the analysis, compliance improvement went from +43% to +56%.
James Spader likes effect sizes of medication adherence interventions!
Being poor, having higher medication costs, lack of insurance
Depression, cognitive impairment
Asymptomatic disease, side effects of medications, complex treatment regimens
Effect sizes
Informational interventions are cognitive strategies designed to educate and motivate patients by informational means. The premise is that if patients understand their condition, they will feel more in control and be more likely to comply.
No clear association between intervention intensity and effect size for informational interventions.
Behavioral interventions are designed to influence behavior through shaping, reminding, or rewarding desired behavior. Examples include teaching the patient skill-building, using reminder methods, simplifying the dosage schedule, or using rewards and reinforcement. No figure included, and at best, mixed results.
Mixed interventions are a mix between behavioral and informational..
Many of the smaller studies show an improvement in adherence, but not the larger studies.
Comments
Complex interventions are more likely to be effective because they address more of the potential barriers to adherence. However, they are very difficult to duplicate outside of an academic setting.
James Spader likes a pill card for people with low literacy!
Health literacy is a big problem in non-adherence. What if we gave pictograms to poor women?
Research design:
Control: usual care
Experimental 1: pictogram designed by a non-local artist
Experimental 2: pictogram designed by a local artist
Research info:
Research site: Pachcham, Gujarat State, India
Demographics: 80% Muslim, literacy rate 53.5%
Experiment: 137 pregnant women
Adherence measures:
Pill count
Self report: how many times did you take this medication each day? How many pills did you take each time?
Patient was deemed adherent if pill count was correct and self-report was correct.
Regimen complexity:
Dosage form
Dosing frequency
Additional directions
Research stuff
Pictures
Results
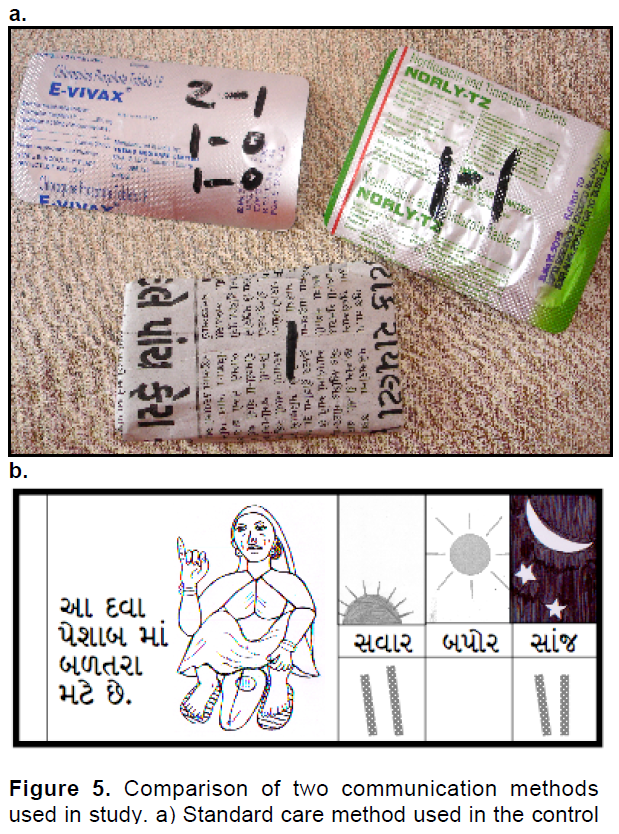
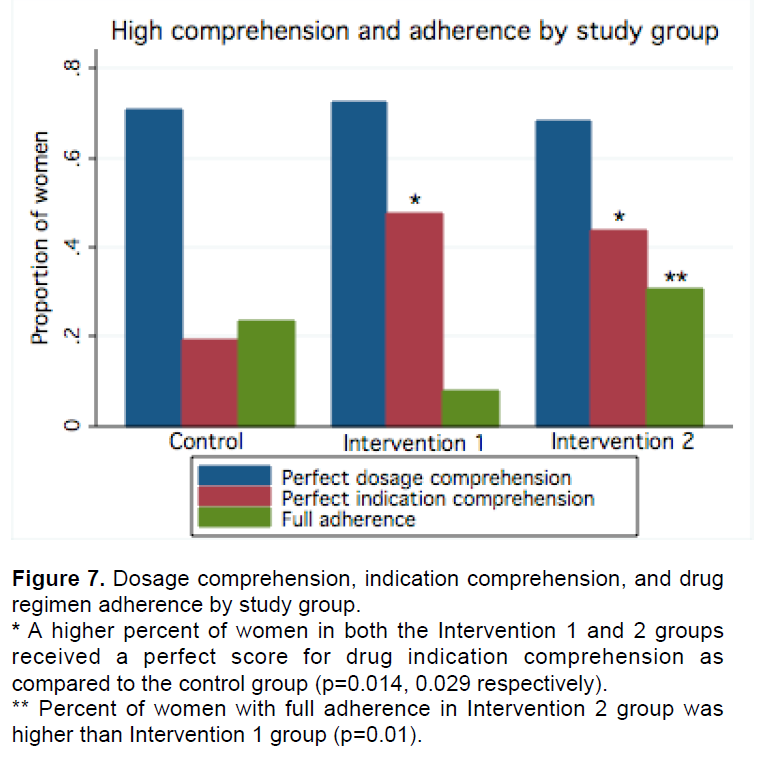
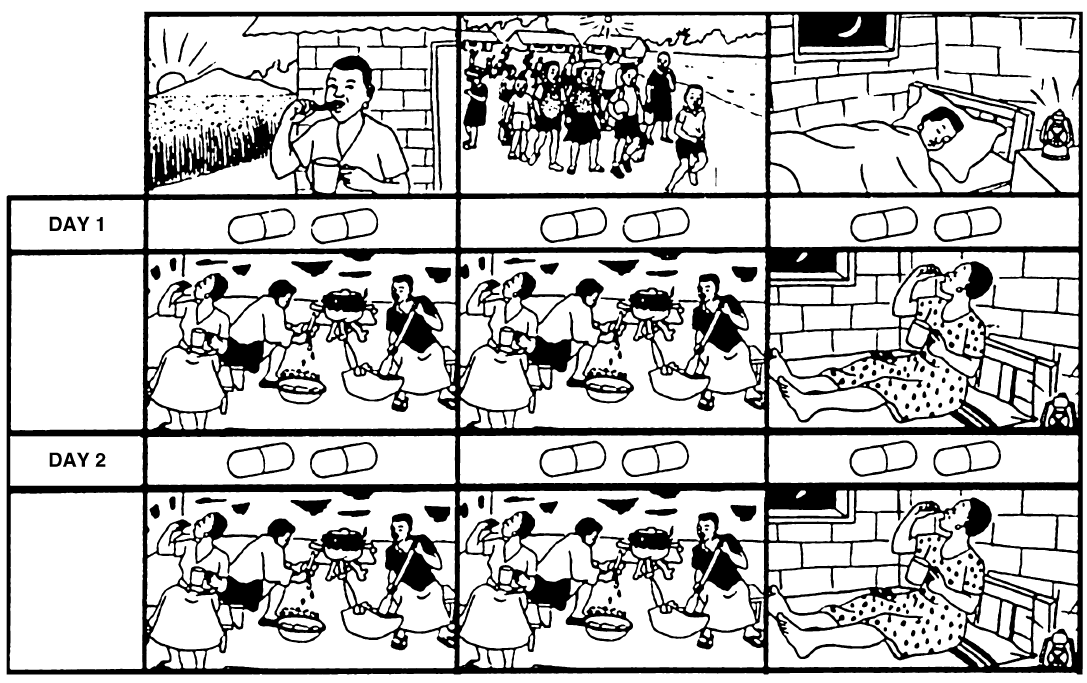
The control group used the top packets, and the experimental groups got the packets and the pill cards in the bottom.
No difference in comprehension between the two pictograms was detected, nor was expected.
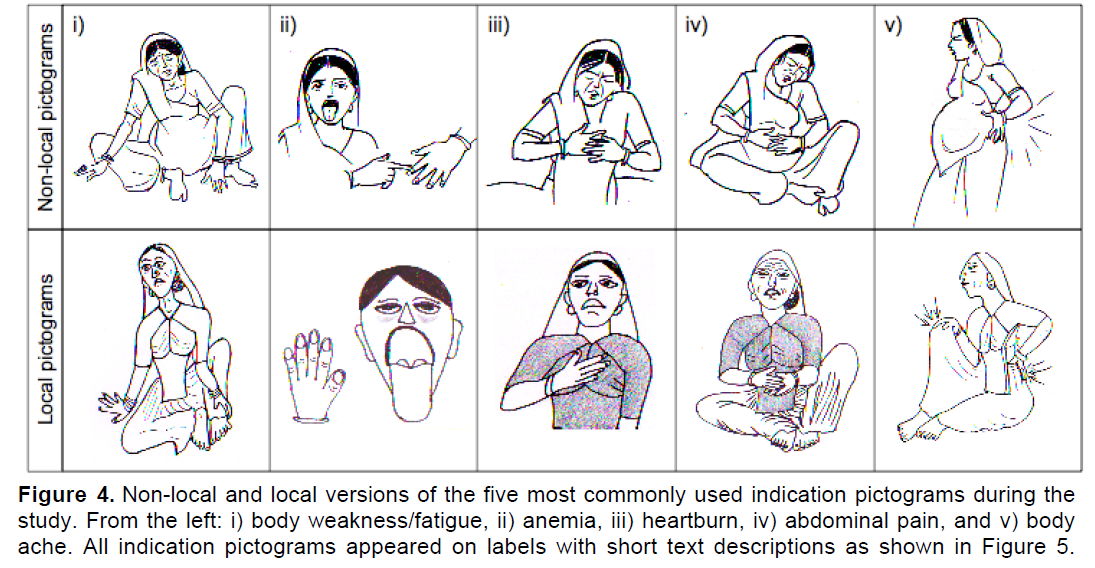
The top pictures are from a non-local artist, and the bottom is from the local artist. Rather horrifying.
No difference in dosage comprehension between the three groups. Women in the experimental groups had higher comprehension of drug indication.
Although ultimately a null result, the group with non-local pictorals had higher adherence than the local pictorals.
Adherence did not differ between control and experimental groups.
Summary
Comprehension of medications is neccessary for adherence, not not sufficient.
The most commonly cited reasons for non-adherence in addition to poor comprehension were side effects, forgetfulness, dissatisfaction with medications, and poor storage of medications. Other women said that they did not think it really mattered whether or not they took the medications forrectly.
James Spader likes the effect of pictures in health comprehension!
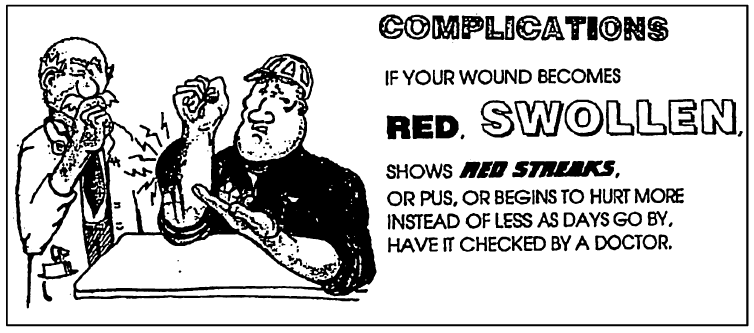
Attention - can pictures make people notice and read a health message?
Yes, patients are more likely to remember medical instructions with pictures than those with only instructions. This effect is even greater for those with a less than high school education.
Medical instructions with pictures.
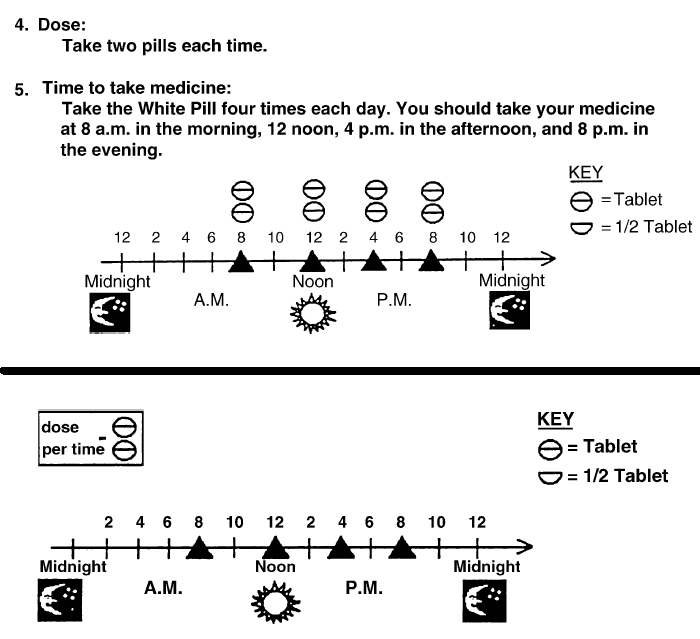
Comprehension - can pictures help people understand a message?
Yes, but only when the pictures are related to the text.
Integrated picture plus text explaining when to take pills on top, and a non-integrated picture on the bottom.
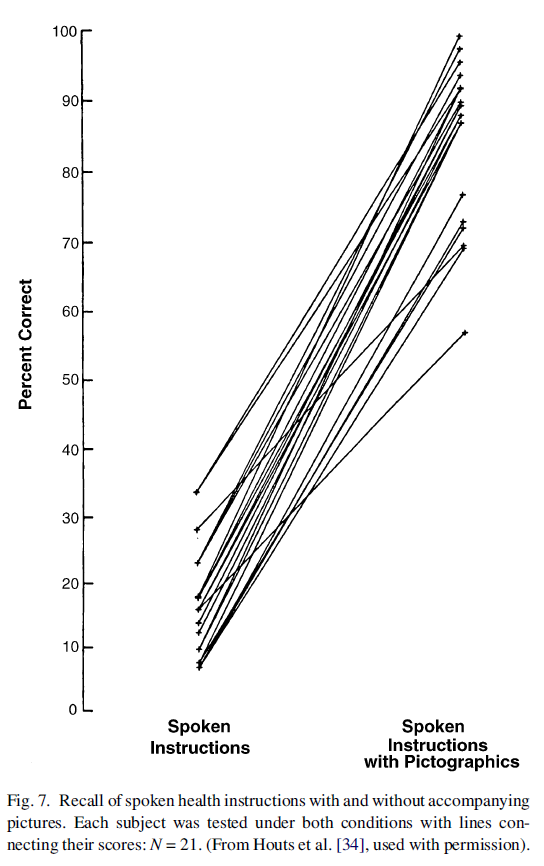
Recall - can pictures help people remember information in health education materials?
Generally pictures help people recall things from memory, but sometimes they are a distraction.
People who had pictures could recall better.
Adherence - will pictures influence medical behavior and intentions?
Pictures added to text does not seem to make people want to adhere better. This relationship is rather complex.
Pictures can change intention and behavior, but it depends on whether the emotional response to it is negative or positive.
Cultural sensitivity and blah blah blah
It will work better on people with low literacy skils
Pillcard for illiterate women in Cameroon.
James Spader likes a 1972 commentary on adherence rates!
Our healthcare system primarily focueses on diagnosis and prescription of therapy for patients. What happens onwards is a matter of chance: whether the prescription is ever filled, whether the patient takes it as directed, whether he takes medications that may interact, etc. If a patient does get eduction, it is in the last hours prior to discharge, when he is still concerned with his hospital bill and how he will pay it.
Adherence
The methods used to measure adherence were of 3 types:
Initial interview followed by an interview in the home of the patient a few days later
Observation of patient taking pills at home
Interview with patients during their visit to the chronic care clinic
Adherence rates were consistently between 25 - 59%. Between 4 - 35% of patients were misusing their medications in such a manner to pose serious threats to their health.
Few characteristics predict the reliability of patients in taking their medication.