Data is a huge resource with an indefinite range of potential uses - Growing accumulation about data, complex data about human biology, health, disease, all derived from the study of people. IT now allows us more ways and more powerful ways to collect, manage, combine, and analyze this data.
Protect the privacy of the individuals - Privacy is fundamentally important to individuals and groups in the maintainence of their identity, their relationships, and their sense of well-being. Biomedical research links and re-use data, so the public interest and private interest are entangled.
What are the morally reasonable expectations about the use of data?
What conditions are required to give sufficient confidence that these expectations will be satisfied?
Compliance with the law cannot guarentee that a use of data is morally acceptable - Protection of privacy cannot be secured simply by anonymization of data or by using data with a consent form. Contemporary data science and its environment is increasingly rich. Effective governance of this data is crucial.
Morally reasonable expectations about the governance and use of data should follow four principles:
The principle of respect for persons
The principle of respect for the established human rights
The principle of participation of those with morally relevant interests
The principle of accounting for decisions
Recommended actions:
Research into the potential harms associated with the abuse of health data, as well of the benefits of responsible data use
Mandatory reporting of privacy breaches affecting individuals to the individuals affected
Anti-blagging measures
Public statement of expectations about who may be given access to health data and for what purposes
Clues
Large amounts of biological data are being extracted, linked, and re-used. Current informational governance measures have not kept pace with these developments.
Conclusion
We need to define a set of morally reasonable expectations about the use of data, and the conditions required to give sufficient confidence that these expectations will be satisfied.
James Spader likes the Nuffield report, part 1: data initiatives!
Definitions
Data initiatives - reusing data in novel contexts and linking them with data from other sources. Watch out for data quality issues!
Data is simply given, while information has meaning.
Changing the context of a data can alter its informational value. For example, genetic data can be used to diagnose or predict disease, but in a different setting, can also be used to identify people or their relationships to others, such as forensics science or paternity tests. Likewise, lifestyle data about alcohol intake or exercise routines can also become framed by mental health or diseases risk in later life.
Primary sources of data
Clinical care data - EMR data, patient reported outcome measures
Clinical trial data - testing for medicines, different interventions to different groups, limited in scale
Observational studies - diseases-specific populations or the public, observed over time. Most famous is the Framingham Heart Study
Imaging data - MRIs, sonograms
Biomarkers - theoretically can be used as identifiers, however, this requires large-scale data linking
Personalized medicine - Next Gen sequencing data, the other "omic" datas
Worry!
Here are some trends to worry about:
Useful information can be extracted from data, in particular, the linking or combining of datasets
A new attitude emerges among researchers: data is a resource that has a wide variety of uses and purposes
Conclusion
The data from biomedical research can influence how people are treated by others, including public authorities, in ethically significant ways
James Spader likes the Nuffield report, part 2: data opprotunities and threats!
Summary
Data in biomedical research can transform efficiencies in services, generate new knowledge, and promote innovation.
However, there is also a risk of musing data leading to harm to individuals and institutions, discrimartory treatment of individals and groups, and fear of state surveillance of citizens.
UK
America has won the first phase of the digital revolution because of connectivity and access to information and efficiency gains, large domestic market size, west-coast entreprenurial culture, and the existence of firms like Google, Amazon, Microsoft, and eBay. But the UK can win the second phase which is able extracting value from publicly-funded data, which belongs to the public.
Data threats
The decisions informed by health data may have both beneficial and harmful effects on individuals or broader groups of people. Also, the potential benefits and harms that could arrise from data may be valued radically differently by different people and by the same people at different times.
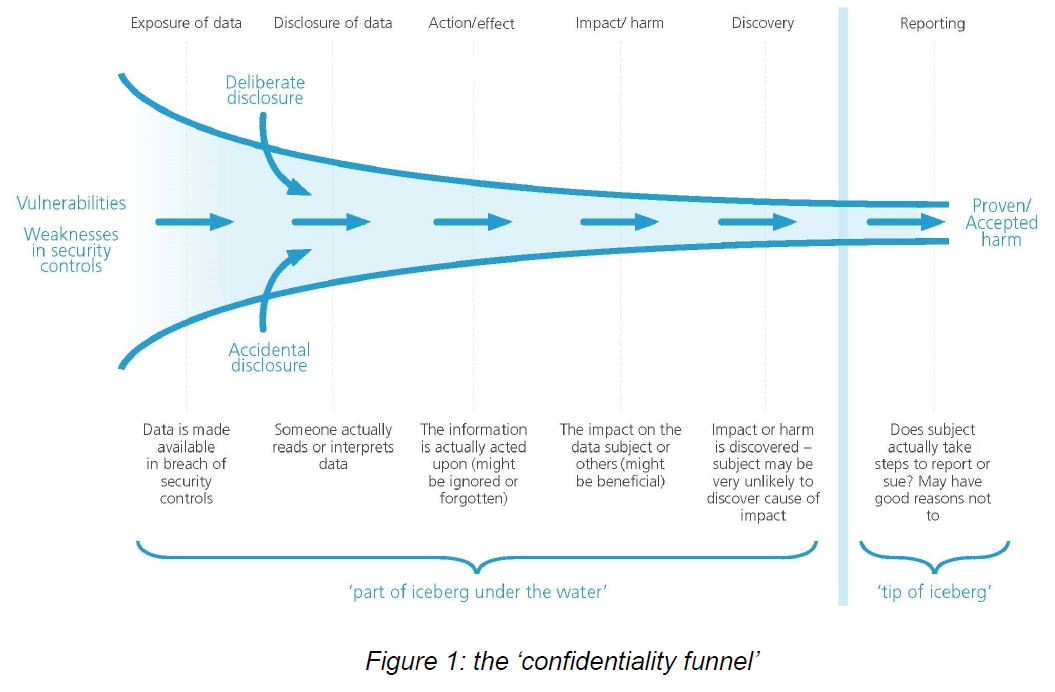
Conclusion
confidentiality funnel.
James Spader likes the challenges of informed consent!
Theoretically, informed consent is the authorization of an activity based on an understand of what that activity entails and in the absense of control by others. In reality, it often falls short of the ideal. The heart of informed consent is the underlying value of respect for the autonomy of person to have goals and the choice to achieve those goals.
Definitions
Ideally, researchers would disclose understandable information to participants, and they would use this information to deliberate and decide whether to authorize or refuse the intervention.
Autonomous authorization by a research participant (what we want)
Legally effective authorization, determined by prevailing rules, policies, and social practices (what we do not want)
Problem
Research consent forms continue to increase in length, complexity, and incorporation of legal language, making them proportionally less likely to be read or understood
Challenges
Harmless activities - The typical proposed solution of requiring "research-like" is burdensome, thwarts improvement efforts, and ultimately, ethically unnecessary. Many learning activities, such as how providers use a checklist, add little risk to patients already using care, involve details of slight interest to patients, and have goals that all patients support. A "simple" informed consent would make sense.
Big, uncertain data - The information generated by advanced technologies is complex, great, and dense, and the anticipated discoveries of expanded research is uncertain in signifiance and of secondary incidental findings. Comprehensively explaining in the advance the elements needed for informed consent is difficult. This is further complicated by low rates of health and science literacy.
More old people - They have Alzheimers
Conclusion
In practice, too much emphasis is given to the written documentation of consent.
James Spader likes new ways of getting informed consent!
The bioethical principle of respect for persons requires that participants are given sufficient information to allow them to make informed and autonomous decisions. However, many participants do not fully understand the information provided and may not be truly informed.
Problem
Consent forms do not disclose everything, are poorly formatted, excessively long, or written above grade reading levels
Advantages of digital media
Computers allow for active participation
Pictorial superiority effect - people remember more when shown a picture than when reading
Computers allow for real-time in-line exercises to test understanding
The information and mode of delivery can be personalized or tailored to each person
Conclusion
Many research participants are unable to understand information using conventional forms. The Office for Human Research Protections (OHRP) is addressing this.
James Spader likes how sometimes informed consent is overkill!
We need more patient engagment in the informed consent process, but we also need to broaden situations in which informed consent is not required or could be waived, such as system level evaluations that today are done without any review or evaluation process at all.
Current view
The current view is that interventional care automatically creates greater risk than control. Even a comparison study of different brands of bath soaps at different hospitals requires extensive institutional review. Or randomizing patients to daytime or nightime dosing of blood pressure medication, even though clinical guidelines do not specify time of day for that dosage. The consent requirements for even low risk studies becomes a significant barrier.
Silly aspects
But system-level investigations of this kind are routinely carried out at hospitals with no review process, formal evaluation, or transparenc anyway, because they are decided at an adminstrative level. for example, nurse-patient ratios are changed by administrators, even though that change can have huge effects on patient care.
Recommendations
Set information about precedents about consent in clinical research with real life examples, and put them on a website so people can see them
Allow for waived informed consent for routine processes and ones that do not increase risk or burden to patients
Broader oversight - risk, treatment, data collection, and analysis should be transparent and informed to patients
Conclusion
Broaden situations in which informed consent is not required, especially hospital-wide evaluations that otherwise would get no evaluation
James Spader likes personalized cancer medicine sold over the internet
Treatment derived from genomic or tumor data is called personalized cancer medicine (PCM). This is increasingly being marketed by for-profit companies, hospitals, and academic centers that create products that personalize, tailor, or individualize care based on genomic or tumor-derived data.
PCM websites emphasis the benefits and downplay the potential limitations of testing: 85% had benefit information, but only 27% included informatin about the limitations of PCM
Costs are variable: Marketeded tests ranged in price from $99 to $13,000. It is questionable whether the tests are covered by insurance.
56% of them were sponsored by a commercial entity, 20% by academic institutions, and 15% by private institutions
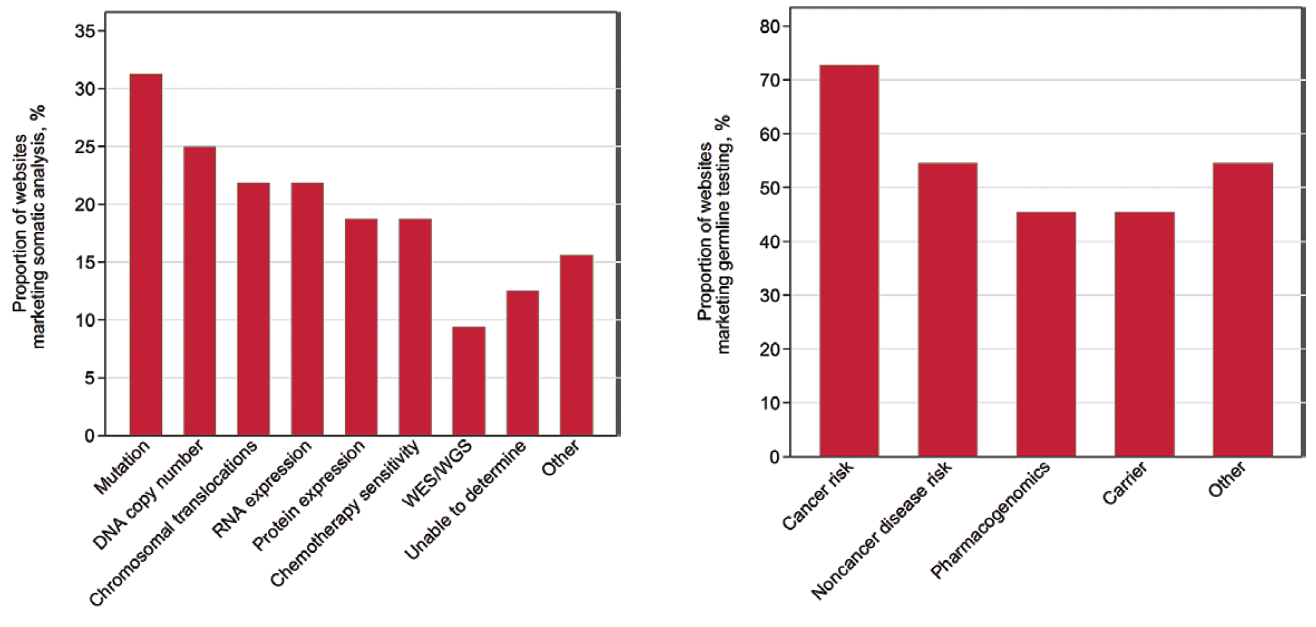
31% offered mutiple PCM services, 58% had somatic analysis, and 20% had germline analysis.
These are the types of somatic and germline testing offered on the internet. WES is whole exome sequencing, and WGS is whole genome sequence.
Marketing claims
The most common marketing claims where:
Tailor/personlize your therapy - 94% of websites - "Personalized oncology means to match the right drug to the right patient at the right time." "By identifying the alterations in each tumors information pathways, molecular profiling enables the individualization of a patients treatment by matching those tumor alterations with one or more drugs."
Identify more effective treatment - 66% of websites - "Our laboratory analyzes your tumors response to 8 - 16 drugs and combinations to identify which treatments will work best to kill your cancer. Why use your body to investigate a drugs effectiveness, when we can garner the results safely and in a timely manner?"
Outcome benefit - 47% of websites - "Through these enhanced treatment options our patients experienced a greater
life expectancy, often with significantly less side effects than standard treatment."
Identify clincal trials - 34% of websites - "A clinical trial matching service ... which helps connect each patient with relevant clinical trials based on each patient’s tumor type and unique tumor molecular profile, clinical history, and personal considerations."
Recommendations
Providers may want to use these marketed tests to teach patients about the clinical validity, clinical utility, and generalizability of the test findings, but if the oncology providers are not well-versed in genomics, it is much harder. Prior studies have shown that there is considerable variation in the education and knowledge of genomics in providers.
Quote from paper: Perhaps companies that market genomic tests over the internet should be required to provide consumerrs with balanced benefit and limitation information, similar to what is required in pharmaceutical marketing.
James Spader likes consumer views on giving their data to companies, research, and healthcare
Patient acceptance of health information exchanges (HIE) is critical for their success. Here are the 3 research questions:
What is the public opinion regarding privacy and security of HIE?
What is the public opinion regarding privacy and security of electronic sharing for research?
Are there differences in views about consenting to electronic data sharing for healthcare purposes v. research purposes?
Background
Two types of networks now exist to support such a structure: a distributed research network (DRN) that allows researchers to access aggregated data, but the data do not leave the local organizations. The second are health information organizations (HIOs), which oversee and govern electronic movement of information such as ePrescribing, lab result reporting, and exchange of care documents.
Research question 1
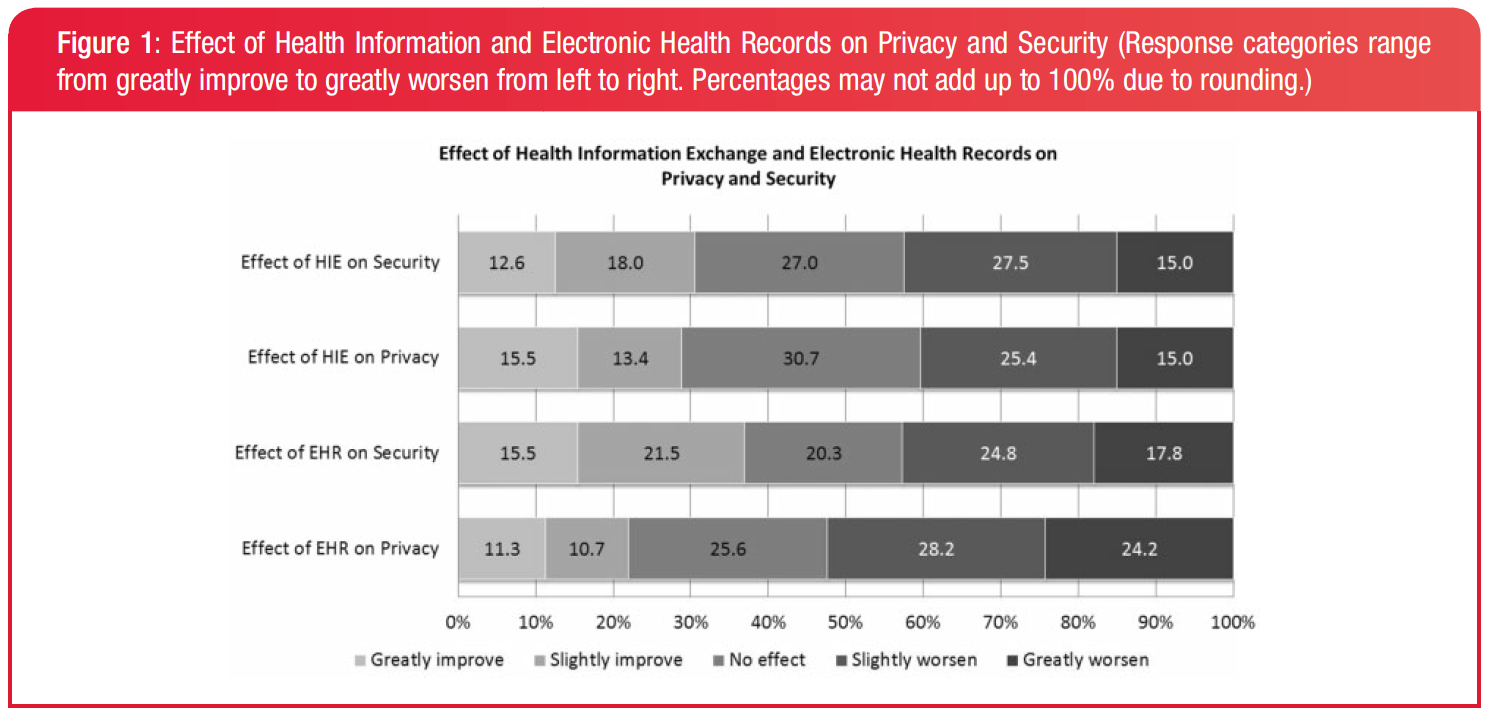
What is the public opinion regarding the privacy and security of electronc health information exchange?
The majority of people have a negative view of the impact of technology on privacy of security, but there is also a substantial minority of people who have the opposite view.
40.3% of respondents think HIE worsens privacy, while 28.9% think it improves privacy. 52.4% think EMRs worsen privacy and 22.0% believe it improves privacy.
Research question 2
What is the public opinion regarding privacy and security of electronic health data sharing for research?
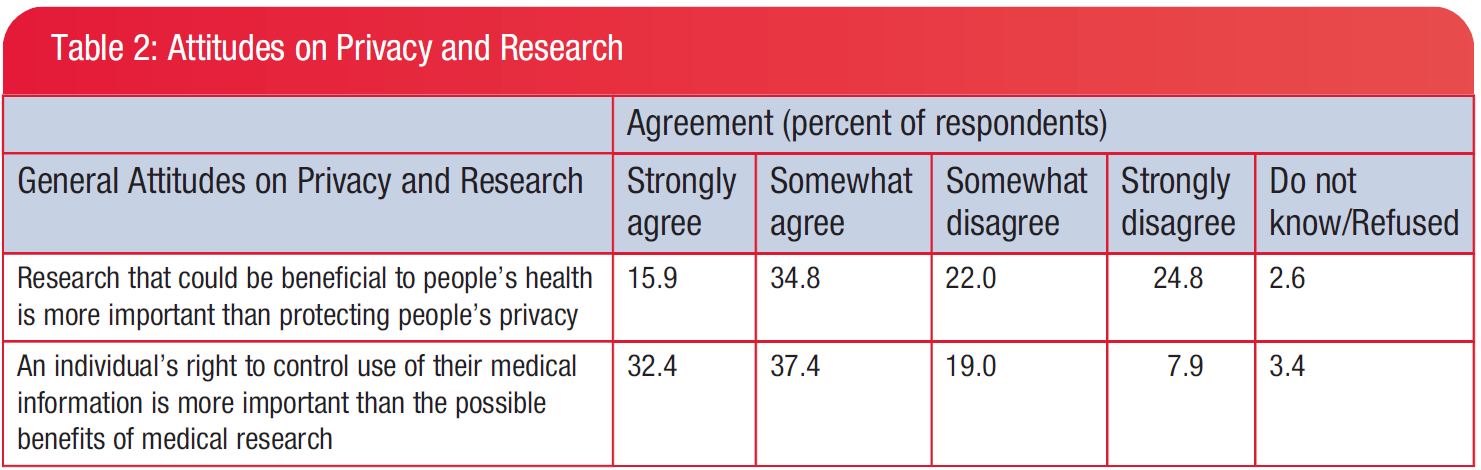
There is roughly equal value put on protecting individual privacy and societal benefit.
50.8% strongly agreed or somewhat agreed that societal benefit was more important than privacy.
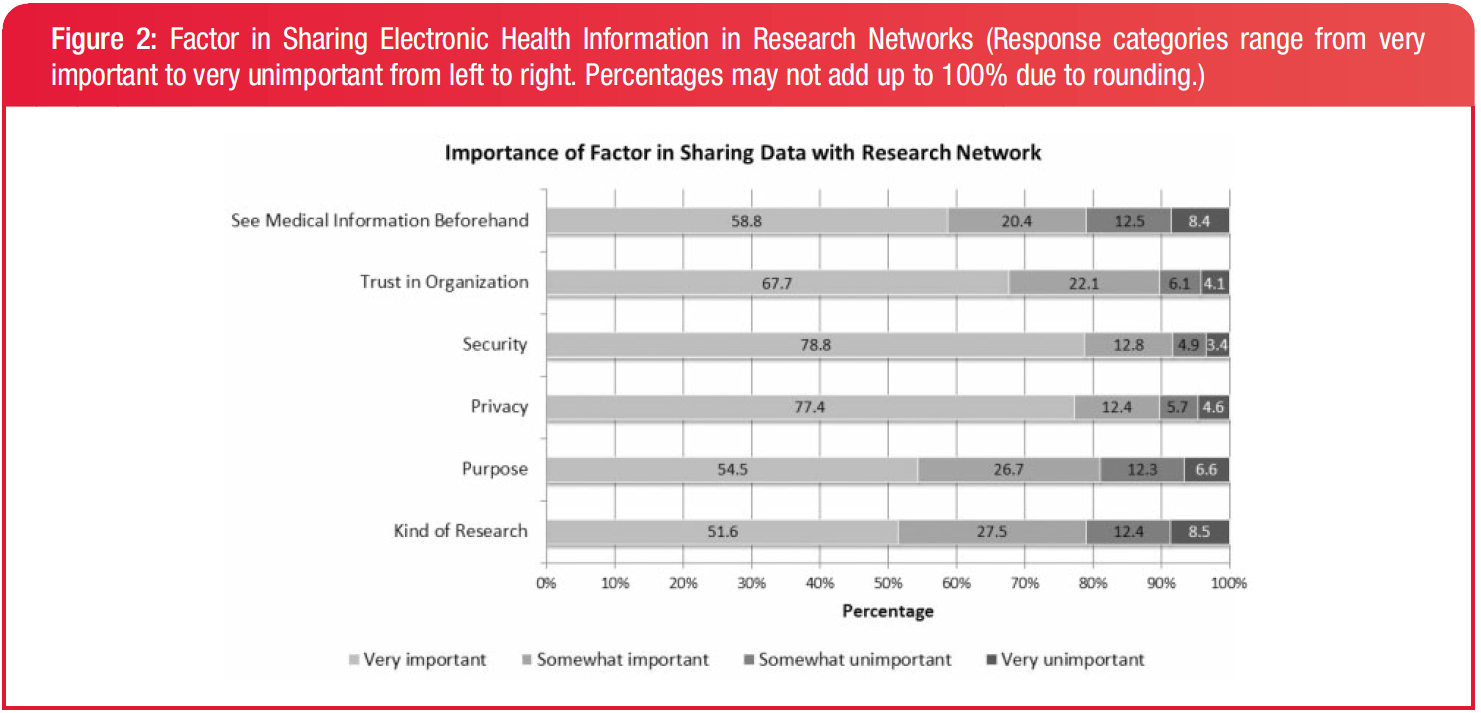
All 6 factors involved in sharing unidentified data through an electronic research network were deemed important.
Security and privacy received the highest ratings and were important to over 3/4 of the respondents.
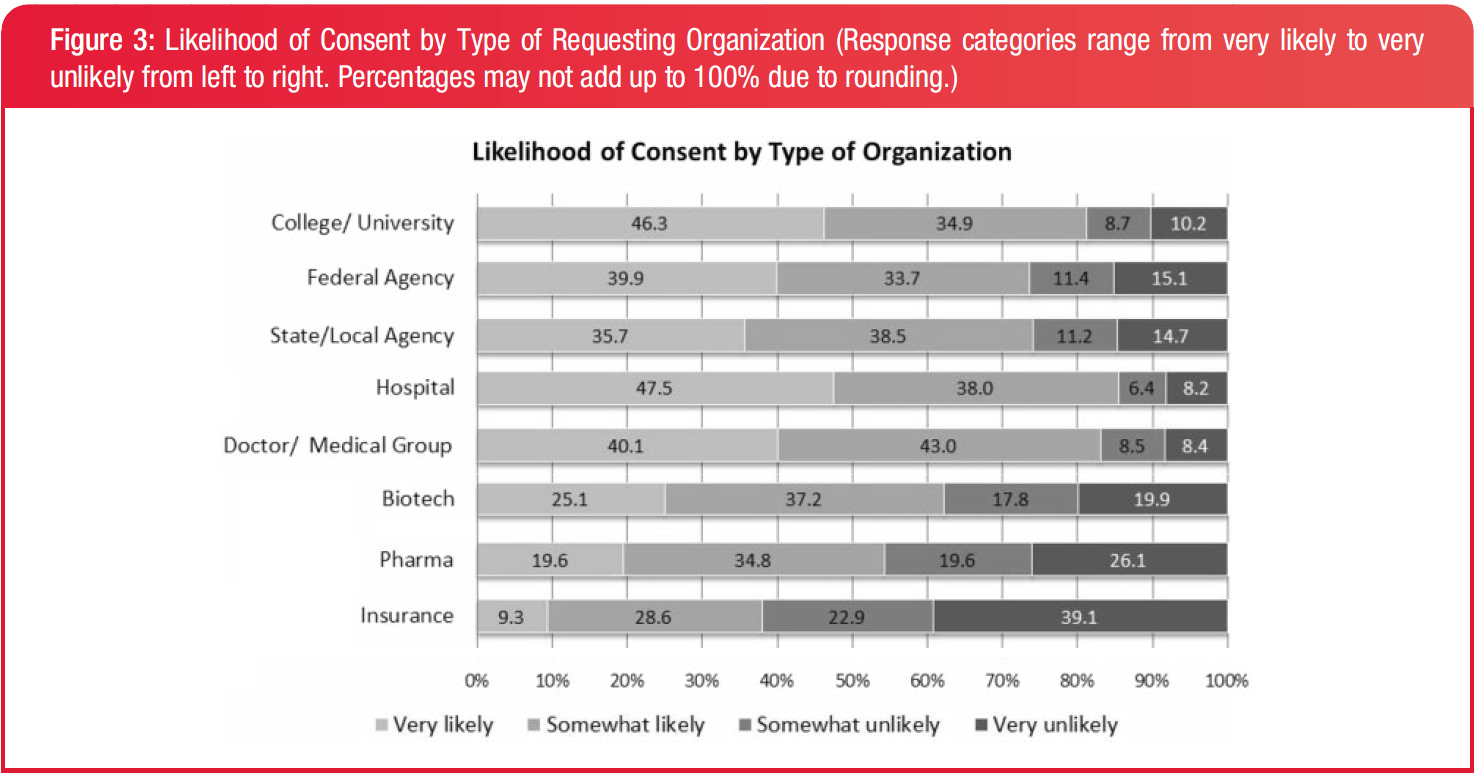
None of the types of organizations had a very high likelihood of consent from the majority. But respondents were mostly likely to consent if asked by a hospital and least likely if asked by an insurance company.
The highest likelihood of consent associated with a hospital or university, followed by doctors and government agencies. The lowest likelihood was associated with biotechnology, pharmaceutical, and insurance companies.
Research question 3
Are there differences in views about consenting to electronic data sharing for healthcare purposes v. research purposes?
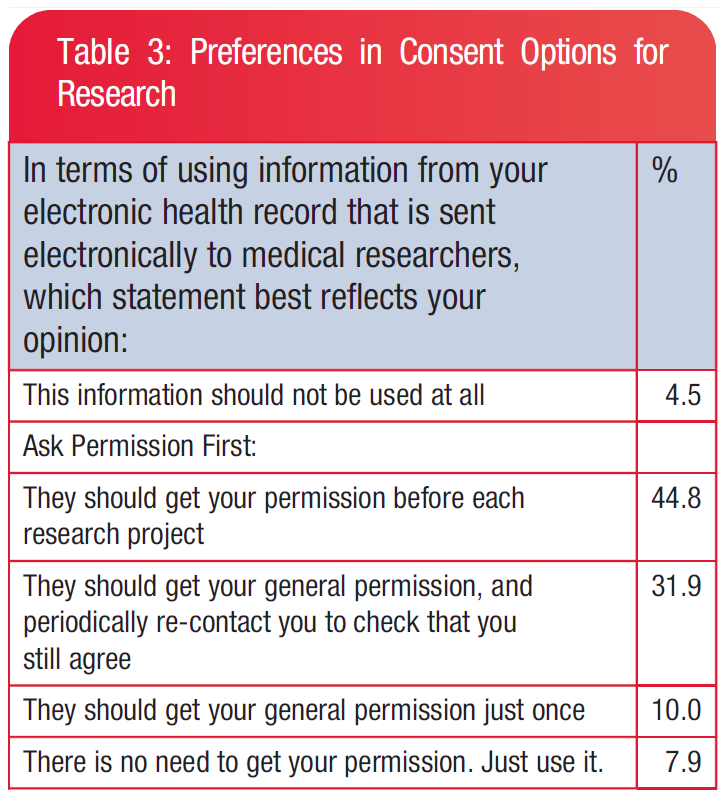
The vast majority of people (86.7%) prefer to be asked for permission first before their data is sent to researchers.
44.8% of people wanted to be asked before their data was used for each project, and 31.9% wanted to be asked periodically.
Additions
There were 3 types of opt-in measures:
Opt out: 11%
Opt in: 23%
Opt in with "break the glass": 66%, their data would be collected but only accessed in emergencies
Conclusion
Consumers are still uncomfortable with the privacy and security of data sharing. There are factors for the likelihood of consenting:
Informed consent: whether or not they are presented with all the information about confidentiality, voluntariness, and individual benefits/risks
Expectation of societal gain from sharing: profits do not count as societal gain
Trust in the organization: people are least likely to share with a biotechnology company, a pharmaceutical company, or an insurance company. They are most likely to share with a hospital or university.
James Spader likes a short overview of giving patients control of their data
Patients: information rightfully belongs to patients, and they should be able to decide what is recorded and who can access it.
Doctors: doctors have a duty to provide their patients with the best possible care, and so they should have complete access to any information needed to provide that care
Clinicians are guests in their patients' lives. They must respect the wishes of their hosts, even when those preferences seem misguided or even when they may compromose the patient's well-being. The first instinct should be to give patients a chance to express their views, and then abide by those as best we can. The patient is the person best positioned to make judgements about the use of their data, and the only persion with the right to make that judgement.
Ethical implications
The principle of individual choice is that "individuals should be provided a reasonable opportunity and capacity to make informed decisions about the collection, use, and disclosure of their individually identifiable health information."
The responsibilities that come with such a right are:
When patient decisions affect the well-being of others, then the rules change. For example, a patient with Ebola cannot restrict access to that information, nor can a substance-abuser withhold information from clinicians who may unwittingly perpetuate that behavior.
By controlling their health information, patients assume responsibility for the consequences of their choices. They cannot hold caretakers legally or professionally liable for negative outcomes that stem from information that was restricted from view. However, patients are not fully fully informed of what is contained in their EHR and who has access to it.
Technological implications
In 1914, the courts ruled that physicians cannot perform surgery on a patient without consent. Since then, informed consent has been de rigueur in hospitals and medicine. However, informed consent of control of EMR data is difficult as of now. Simply knowing what is in a health record does not mean patients know why clinicians need certain information, as a clinician's ways are often non-linear. A patient's decision to withhold HIV data may have consequences that neither the patient nor clinician could have anticipated.
Choices for information restriction:
No restrictions - most will probably pick this
Restrict sensitive conditions for certain providers
Hide all of their data, or be notified when the physician wants to access their record
Regardless of choice, patients should be able to revist their choice periodically
Physicians should also be able to "break the glass" -- access the medical record in cases of emergency.
Recommendations
Technology-wise:
Develop further the technology and processes for informing patients of their choices
Put technologies into practice
Observe consequences
Policy-wise:
Research how to inform patients
Support their choices
Understand that consequences for their care is essential
James Spader likes extreme views of patient-centerednsess
I suggest that we should without equivocation make patient-centeredness a primary quality dimension all its own, even when it does not contribute to the technical safety and effectiveness of care. - Donald Berwick
Summary
Patient-centeredness in healthcare will require a disruptive shift in control and power, out of the hands of people who give care and into the hands of people who receive it. This consumerist view of quality care differs from the classical, professional definition of quality.
Definitions
IOM 1998: the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge
IOM 2000: Ended up as "the patient is the source of control," but started off as "patients have all the control."
Professionalism puts the judgment of quality in the hands of professionals. "Trust us; we know best what will help you."
Consumerism puts that judgement power into the hands of consumers. "Let us know what you need and want, and that is what we will offer."
Patient-centeredness
The three maximus for patient-centeredness are:
The needs of the patient come first
Nothing about me without me
Every patient is the only patient
A new definition by Berwick is: The experience (to the extent the informed, individual patient desires it) of transparency, individualization, recognition, respect, dignity, and choice in all matters, without exception, related to one's person, circumstances, and relationships in health care. Examples include:'
Hospitals would have no restrictions on visiting - no restrictions of place or time or person, except restrictions chosen by and under the control of each individual patient
Patients would determine what food they eat and what clothes they wear in hospitals (to the extent that health status allows)
Patients and family members would participate in rounds
Medical records would belong to patients. Clinicians, rather than patients, would need to have permission to gain access to them
Objections
Evidence-based medicine sometimes must take a back seat: Leaving the choice ultimately up to the patient and family means that evidence-based medicine may sometimes take a back seat. So should a patients wants for an MRI override professional judgement on whether an MRI is needed. Basically, yes. Better to take the risk of overuse along with the burden of giving real meaning to the phrase, "a fully informed patient." If over time, a lot of patients emerge scientifically unwise, such as choosing needless MRIs, then we should improve our messages and patient education processes.
Physicians as a steward of social resources: Public policy is the right place for getting the aggregate data of needs and wants for informed social policy.
Clinician needs and wants: Does patient-centeredness require physicians to become martyrs? Only if you become emotionally detached from your patients. Physicians expent enormous energy when they enforce restrictive rules and lose touch with the underlying needs of their patients. If you were more attune to your feelings and your patient's feelings, maybe you'd empathize more with them.
Recommendations
"They gave me all the care of needed and wanted exactly when and how I needed and wanted it": Patient and family-centered care is a dimension of quality in its own right, and not just through its effect on health status and outcomes
Patients have control about decisions about care in all its aspects
Extend transparency to all aspects of care, including science, costs, outcomes, processes, and errors
Use individualization and customization as design targets
Train young professionals with emotional intelligence, as well as mindfulness, inquiry, and dialouge
Doctors are afraid that extreme patient-centeredness may be tiring. However, Kaiser Permanente saw visit rates fall when email care was rolled out. So maybe their workload would decrease anyway.
Why has patient privacy been a thing since the times of the Hippocratic Oath?
Trust is central to achieving health outcomes, not least is the trust that health information revealed to the provider will be kept confidential
If patient privacy is insufficient, some patients will avoid care altogether: HIV, mental health, adolescents
Even when patients do seek care despite privacy concerns, they may withhold health information
The most frequent reason (30%, or 5.4 million people) that people decline participate in health research is the concern that their personal information would not be kept private and confidential. This even beats out the concern that the process would be risky!
Counterpoint
The quality of health care is directly affected by providers's ability to make the right clinical decisions, which requires the right information at the right time.
Many physicians have strong negative feelings about patients having such control over data. Conerns include chagrin, errors in judgement, and medical liability
Sloppy, unsafe care: All information in the patient's record has relevance in primary care. Maybe not specialist care
Medicolegal liability: Even if only 1% of patients would not share everything with a doctor, how can you treat that 1%?
Patients have to accept that health care is an information business, and the best care requires information
Response
What exactly is the "right clinical information?": we do not know. Even today with incomplete records, the "right clinical information" is only the information the patient is willing to admit. Doctors provide excellent care nonetheless.
Data deluge: providers already do not have time to process all the patient data they have access to
Besides, maybe you should try talking to your patient instead of trying to get at their data against their will
James Spader does not like that patient satisfaction is correlated with bad health outcomes
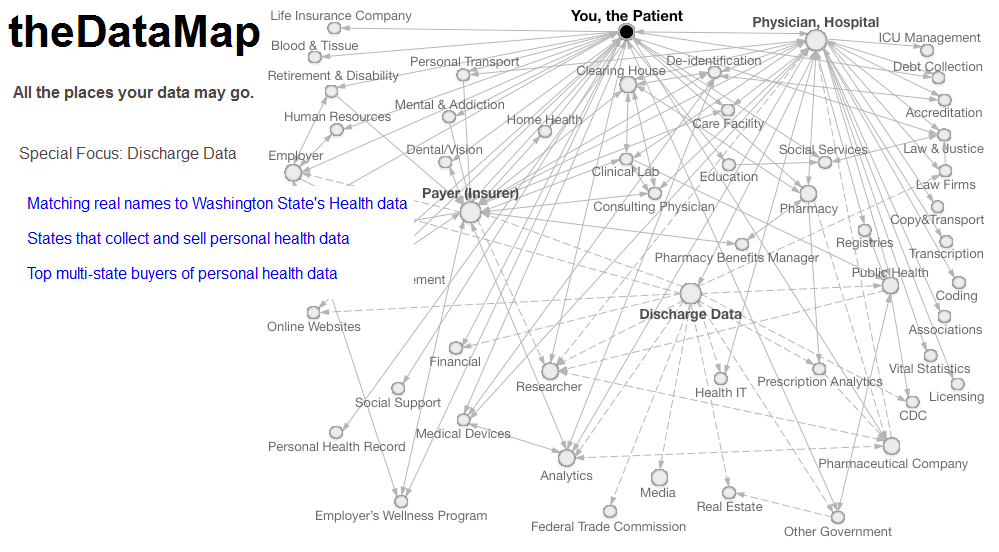
Where is your data going?
The Data Map shows that no one really knows how widely their health data is actually shared.
Results
Know what is in an EHR: 90% do not
Have access to information in an EHR: 90% do not have access to information in EHR
Believes they know who can view EHR: 97% do not know who can view the EHR
Desire access to own medical record: 100% desire access to their own medical record
Desire control over access to health information: 100% desire control over access to medical record
Would like notification when EHR is accessed: 80% would like to be notified when EHR is accessed
Methods of access control: 93% would like to grant permission as a form of access control, 30% would like to restrict or block certain information, and 20% would like time limits or temporal control
Access on "need to know": 83% spontaneously mentioned it
Stated that they do not know what doctors need to access: 80% did not spontaneously mention it
Recommendations
Easy patient access to EHR data: individual access,or ensuring that people have access to data collected about them, is a core principle of fair information practice. However, only one third of US doctors think patients should have full acess to their EHR information
Summary of what is currently shared with whom: No patients knew the reality of how widely their information was shared
Provide granular, hierarchical control: People should be able to let us know what information they want shared with whom
Time-based controls: Patients should be able to restrict certain information based on the time it was collected
Contextual privacy controls: Restrict access based on the medical account, whether it is an appointment, in a display, in a specialist, etc.
Access notification: active monitoring to see if there is unauthorized access
Conclusion
Patient access to EHR can be a double-edged sword. On one hand, giving patients control may mean they are more willing to disclose information. But restricting information may also reduce the benefits of an EHR as a coordination and communication tool.












{kind=link}
{kind=link}
{kind=link}