Quantified self - recording and reporting information about behaviors can motivate people toward better habits and health
How to change behavior
1. Hard way: turn external motivations into internal ones
2. Also a hard way: sustain external motivation
Feedback loops
Use the experience of past rewards and prospect of future rewards
Inform people what they would have won had they been adherent to a new behavior
Gaps
Requirement
Gap
Solution
Person must be motivated enough to want a device, and be able to afford it
Wearable devices are used by people who need them least: early-adopters, people younger than 35, and who make more than $100,000
The people who have most to gain are those who are older and less affluent. Make devices more affordable, or make new funding mechanisms, such as making it part of insurance or a prescription
Person needs to remember to wear the device and charge it regularly
More than half of people who purchase a wearable device stop using it, and a third of these people quit <6 months
Leverage smartphones: Lots of people have them, and they carry their phones around everywhere. Data is already transmitted passively.
Device needs to accurately track behavior
Pedometers are doing a great job, but heart rate and sleep cycle monitors have not been validated.
Wearable devices help create a better feedback loop than a home device alone. For example, a watch that tells you to take your pills can supplement a medical box that glows red when you have not opened it.
Information must be presented to the user that is easily understood so it can motivate and sustain further action
Sustaining change is easy for the already motivated, but difficult for those with chronic health problems. Workplace wellness programs tend to reward the highly motivated and discourage the majority of others who need them most.
Team-based wellness programs provide peer support and a sense of accountability rather than rewarding a new power individuals.
Take home message
Engagement strategies drive the success of devices, not the technological features. These are persuasive human behavior feedback loops: encouragement, social competition, collaboration.
James Spader likes knowing what marketers are thinking!
Use the experience of past rewards and prospect of future rewards
Inform people what they would have won had they been adherent to a new behavior
Foundation
Question
Answer
What inferences do users make about design intent?
They can infer relevent intentions (this product was intended for brand recognition or personal attachment) and intentions based on contraint and limited resources (they were in a hurry to release this product, they added this feature to differentiate from the other model).
Which factors affect these inferences?
The user, the product, and their relationship affects what the user thinks the product does. Old people might infer more intentions because they have a lifetime of experience, but maybe younger people are more likely because they are cynical. The product itself only raises attention if it malfunctions and makes the user wonder about how it works. Lastly, strongly interested users are more likely to infer intentions because they think about the product more.
What are the effects of these inferences?
The effect depends on whether the user feels tricked/exploited versus being protected/appreciated. The effect can be modified if features of the product can reinforce contradict each other.
Take home message
Ask users why they think a feature is the way it is, and whether they are aware is was designed. You may be surprised by the answers!
James Spader likes knowing whether the foundation of this field are valid!
Persuasive technology: technology can affect people, their attitudes and motivations, and thusly, their behavior. Focuses more on communicative persuasion.
Gamification: Same as above, but focuses more on intrinsic motivations through gameful experiences
Question
Do persuasive stimuli actually affect psychological outcomes and behavioral outcomes? Do these technologies really form, alter, or reinforce attitudes, behaviors, or complying?
Results
Things
Results
Type of results
52/95 (54.7%) were positive
36/95 (37.9%) were partially positive
only 7/95 (7%) were negative or neutral
Quantitative v. qualitiatve
52/95 (54.7%) used all quantitative methods
15/95 (15.8%) used only qualitiative
28/95 (29.5%) used both
Most popular persuasive features
Visual or audio feedback (26.3%)
Social support, comparisons, feedback, interaction, sharing (23.1%)
Progress (16.8%), Persuasive messages and reminders (16.8%)
Objectives and goals (15.7%)
Rewards, credits, points, and achievements (15.7%)
Most popular psychological outcomes
Engagment/encouragement (29.5%)
Motivation (25.2%)
Awareness (22.1%)
Most popular genres
Health, exercise (47.4%)
Ecological consumption (21.1%)
Education/learning (10.5%)
Take home message
Most persuasive technologies are implemented in whch people are willing to take part in the target activities, but find it difficult to start or continue working toward them. Note: few studies took general attitude as a variable
James Spader likes finding out how people use a medication adherence app!
Most mHealth interventions study a particular black box appliction compared to a situation with no black box application. This study presents a way to directly assess usage and acceptance of a mobile technology.
Cool things
Small data - people mainly need technology to help them make sense of their health condition, and to offer actionable steps
Debunked: digital divide - the idea of a digital divide, which says that older users are less likely to use digital technology, was not shown to be true for this app. Users who were older and took more pills (polypharmacy) used the app longer and more times per day.
The app, iNephro Medication Plan, was free for download from the Apple app store. It was for tracking pills. Afterwards, they collected the demographic data of each user. They had 1708 records. 69% of them used the app for more than one day.
Functions
Medication regimen, reminder and push-notifications, vital signs could be graphically represented
Results
Corelations
Interpretation
Age and longer usage
50% of users under 21 used the app for more than one day, but 70% of users over 40 did
Actually taking medications and longer usage
42% of users who did not take any drugs stopped after one day, but only 25% to 30% of users who did take medications did. The app also had functions like weight tracking, so that is why not everyone stopped.
Polypharmacy
Number of diseases and number of pills increased usage intensity
Final
Unless elderly people see a clear benefit for themselves, they are less likely to adopt the new technology.
James Spader likes designing a self-monitoring system!
Mary uses the PAL system to record activities from her PDA, which records her thoughts and reactions throughout the day, which is put into a daily story view
Self-awareness
Mary is unusally tired and sees that she has lots of meetings and skipped lunch
Self-understanding
Her colleague, George, kept interrupting her presentation, as usual, which annoyed her. She can talk to her doctor about this, or yell at George.
Theory
Principle
Issues
Information gathering
What information is relevant
Balance between too much and too little
Allow users to enter data into system
Information processing
Balance between too little and too much processing
Let users help process information if they want
Information presentation
Let users interact with the display
Allow users to understand how it was processed
Final
Lessons learned:
It is unrealistic to assume people will remember to switch on devices, much less wear them all day
It is not comfortable to wear these devices all day
People will use devices based on how exciting they expect their day to be
James Spader likes research in quantified health!
Here is a running list of interesting things in quantified health
Cool things
A running list of interesting Eric Topol ideas or sayings.
Internet of Medical Things (IoMT) - smartphones, sensors, and other medicial intelligence will be distributed in the cloud and all around the house
Peer to Peer (P2P) medicine - patients can connect to other patients and share their problems
Patients are better at understanding risks than physicians - the person bearing the risks and costs of medications and screenings want a larger voice
Not cool things
A running list of criticisms to addresS:
Data security - the usual
Data quality - does the data make sense?
HIE - what to do with so many data sources
Stakeholders - get vendors to pay attention
Money
New center
Samsung and UC San Francisco are setting up the the Center for Digital Health Innovation. Already they have 50,000 people signed up for medical wearables device experiments. That would have normally taken 50 medical clinics and millions of dollars, but they did it only 24 hours. Projects incllude:
Technical validation - input and output, get the devices to actually measure accurately things other than number of steps you took
Comparison against gold standard - make the devices as good at measuring things as medical-grade equipment
"Creative" clinical trials - who knows??? maybe novel vital signs?
Although physical activity apps are super popular, most are not explicitly grounded in health behavior theories and the vast majority have not been evaluated by scientific methods. Some however have been at least been evaluated with at least their fidelity to recommendations for weight loss and obesity prevention.
The most well-established technique for bridging the intetion-behavior gap, "action-planning," is relatively rare in physical activity apps. Only 6 of 200, or 4% of apps had it. Note: find out what action planning is
Features
Most common overall
Most common in paid apps
Providing instructions on how to perform a behavior
Modeling/demonstrating behavior
Providing feedback on performance
Goal setting for behavior
Social support, approval from others
Feedback on performance
Social support
Setting graded tasks
Providing information on where and when to perform behavior
James Spader likes creating an action plan for exercise!
Action planning is a strategy in self-regulation. It consists of 4 element:
What - What type of activity they will engage in
Where - Where they will particpate in activity
When - When they will participate in activity
How - Number of days that they will engage in activity
Experiment 1
Research design:
Control group: Messaged about physical activity and asked to write an action plan
Experimental group: Messaged about physical activity, and planning information, and asked to write an action plan
Outcomes were:
Whether or not they actually wrote an action plan
The quality of the action plan
Results:
No difference number of action plans created between control and experimental group
However, the experimental group had a much higher quality of action plans
Experiment 2
Research design:
Control group: gain-framed action planning message (By making a detailed physical activity plan, you are more likely to be regularly active and ultimately meet the physical activity guidelines)
Experimental group: loss-framed action planning message (Failing to detail your plan increases the likelihood of falling short of being regularly active and working toward physical activity guidelines)
Outcomes were:
Whether or not they actually wrote an action plan
The quality of the action plan
Results:
Week 1, there were no differences in action plan creation. In week 2, the gain-framed message group sustained their rate of planning, while the loss-framed group had a significant decrease in the rate of action planning.
No difference in quality of action plans for either group
James Spader likes knowing if mobile health apps are backed by theory!
This is a review of the theoretical basis of mobile health behavior interventions. They found out that although some interventions did have a theoretical basis, they have mostly been used to tailor the intervention with pre-intervention factors, but have not been used to adapt the intervention to the individual over the course of the intervention.
Based on input data, interventions should be able to adapt both the content and the timing of the interventions. These intra-individual dynamic regulatory processes are a poor fit with the static, linear nature of current theories.
Just-in-time interventions adjust based on data obtained during the course of the intervention, which can stretch over minutes, hours, or days. This is in contrast to real-time which refers to input occuring at the time of recording.
Results
Smoking cessation interventions were based on:
Social Cognitive Theory
Self-Regulation theory
other cognitive-behavioral theories
Output is mostly text messages. The content of the messages based on theory and told the user to manage their urges and messages of social support. Although there were significant short-term gains, there insufficient evidence for long-term effects.
Weight-loss interventions were based on:
Social Cognitive Theory
Output ranged from non-tailored weekly informational text messages to real-time monitoring and customized, computer-algorithm generated text messages based on input. Most of the output was text, but some had some graphic comparisons to targets/goals. Most show modest but significant outcomes for weight loss. More senors mean more precise and richer measures of dietary and physical acvitiy detection in the future.
Treatment adherence studies did not have a theoretical basis
Two studies addressed medication adherence, specifically in HIV. Both used two-way pagers, which I guess is like a primitive cell-phone. I think. These pagers would remind patients and they used a smart pill box to track their pill-taking. Both studies tailored their intervetion based on the medication regimen of each patient, but no adjustments were made during the course of the intervention.
Most of the disease management interventions were for diabetes. They did not have a theoretical basis, but maybe it is because diabetes already has evidence-based guidelines for managing both type I and type II. However, many of these interventions went further than medication adjustments: physical activity, medication adherence, food intake, etc. so using a theory to inform those elements could have improved outcomes
Most just-in-time adjustments were made manually. We need to get better at automating disease managment, however, the bottleneck is the data entry burden on the patient. Automatica transmission of testing data alleviates that somewhat. These interventions do improve treatment outcomes, and can serve as a basis for a more comprehensive and automated intervention.
Summary
Inputs
Outputs
Most common currently:
Text messaging (SMS)
Future possible inputs:
Voice
Text
Video via camera phone
Medical devices like glucometers
Most common outputs
Text messaging (SMS)
Audio voice and video
Future possible outputs:
Data display of outputs: progress charts, animation, videos, games
Two-way interactions are sadly lacking, which is too bad, because that is the only way to get the just-in-time interventions. Disease managment and weight loss interventions primarily rely on input while adherence and smoking cessation interventions rely mostly on output.
Inputs have a futher problem: many use user-initiated or unprompted inputs even though prompted inputs have been shown to be better. Even a basic confirmation message, an important feature for continued input, was often missing. The interventions that sent tailored messages often did encourage users to send a reply back.
"Just-in-time"
None of the adherence interventions made just-in-time adjustsments, and none obtained the input necessary to make treatment adjustsments.
The disease management interventions had adjustsments, but relied on manual adjustments made by a health care professional. Could standard treatment algorithms be used for to automate the simpler cases, and leave the complex ones to professionals?
Smoking and weight loss had interactivity, but was limited to additional text message assistance or adjustments to exercise and diet inputs.
Engineering I
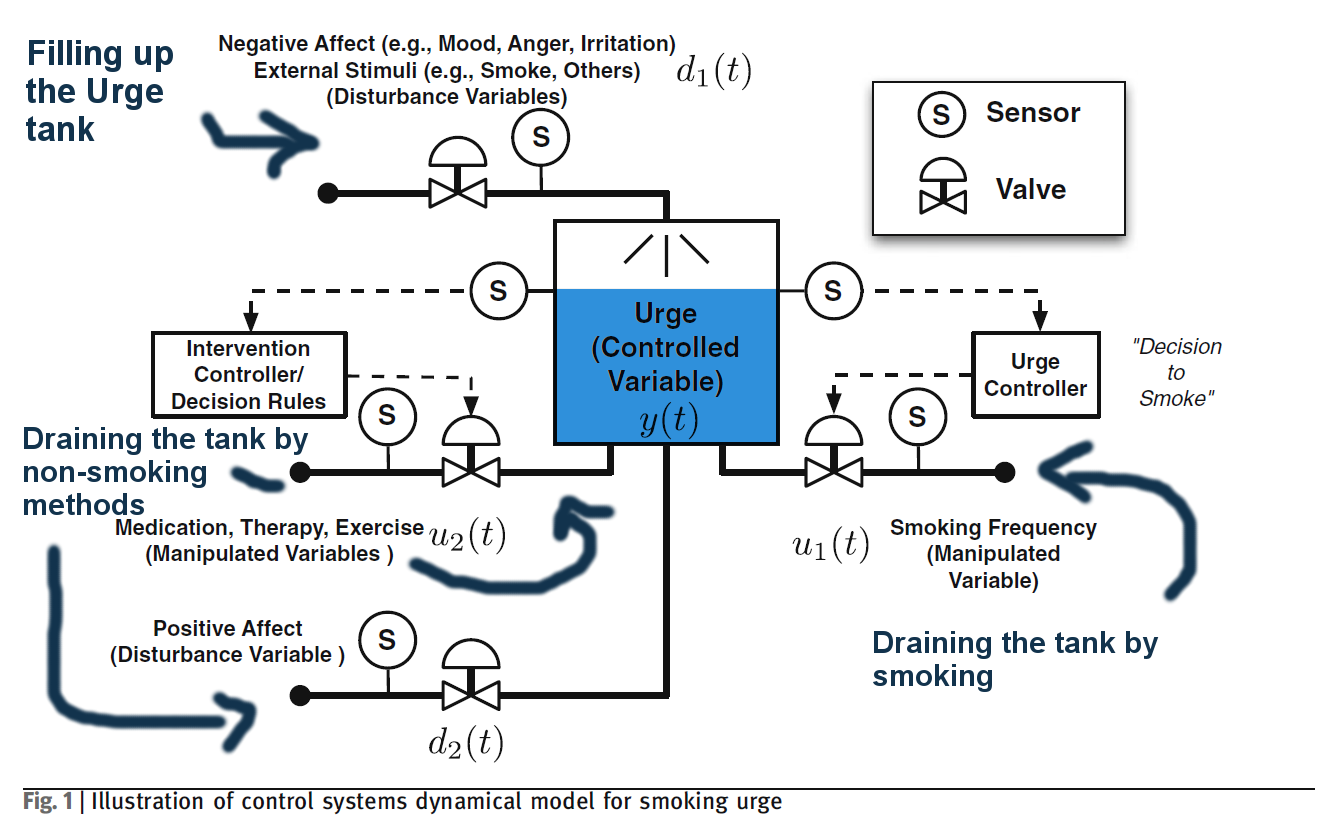
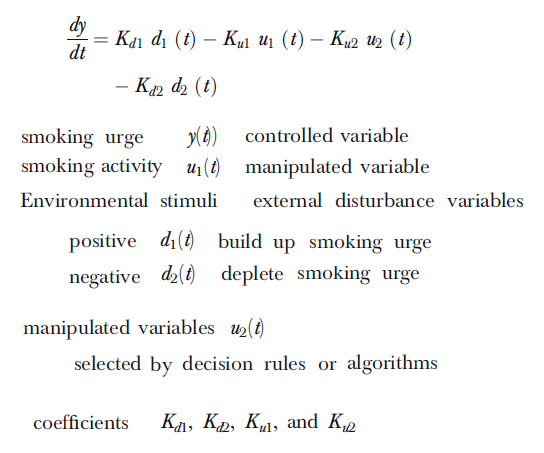
control system dynamic model for smoking This is a rather nice engineering model of health behavior applications. The idea here is that there is a is a vat of "urge to smoke" fluids that is filled up negative environmental occurances, and at a certain threshhold, the person can reduce the urge to smoke by either smoking, choosing a non-smoking alternative, or positive environmental occurences.
relevant equations
Engineering II
Control systems engineering examines how to influence dynamic systems to achieve a desired outcome. These systems are multiple variables that can be manipulated, and have time-varying, non-linear processes. These feedback control systems have the potential to reshape health behavior theories.
Final
Health behavior theories and models need to be able to guide the development of complex interventions that rapidly and iteratively change in response to users requests. Let us try engineering stuff, like control system engineering!
James Spader likes a web-based app for lower back pain!
Non-specific low back pain (NLBP) is temporary back pain with no medical signs of a serious underlying condition. Fitback is an online program, available on desktop and mobile phones, that provides a self-management intervention that uses tailoring, gain-gramed messages, and self-monitoring of cognitive and behavioral strategies to improve self-care and back pain. It was based on social cognitive theory (SCT) and the Theory of Planned Behavior (TPB).
The intervention consisted of:
pain and activity self-monitoring tool
weekly gain-gramed text and video messages, segmetted for sitters, standers, and lifters
activity picker (rest and relief, mindfulness, general fitness, and back-specific stretching)
Results
Users of the Fitback program were less likely to be experiencing back pain, experiencing general pain, more likely to have a high functionality and quality of life, and engage in healthy behaviors after 4 months than the control or alternative care program.
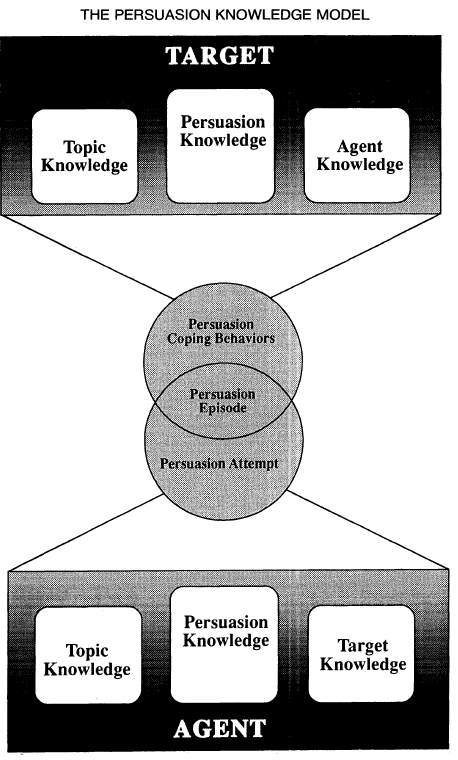
James Spader likes the Persuasion Knowledge Model!
The Persuasion Knowledge Model (PKM) describes how the persuasion knowledge of a person influences their responses to persuasion attempts.
Definitions
Target - people for whom a persuasion attempt is intended
Agent - whomever a target identifies as being responsible for the persuasion attempt
Attempt - the target's perception of an agent's behavior in presenting information designed to influence belives, attitudes, or actions
Cope - how the participants pursue their own goals, maintain control, and select response tactics
Content
Here are the main perceived causal structures:
Psychological mediators - consumers think psychological events are internal causes
Marketer tactics - causal links between a persuasion tactic and psychological activity
Coping tactics - users believe they can manage thier own cognitive, emotional, or physical abilities
Effectiveness of marketer tactics - some tactics are simply thought of as powerful
Marketer's goals verus one's own goals - consumers understand that the the goal of a salesperson is to influence beliefs about a product
Valid attitudes
Consumers seek to hold valid attitudes about the individuals and organizations that they expect to do business with.
Consumers are aware that a company selects sales agents with certain characteristics, personalities, and trains them in a certain way. However, they are also aware individual salespeople have some leeway in how to execute persuastion attempts.
An agent who is directly responsible for designing or developing the product has more sway with a consumer
If a consumer does not have a lot of topic knowledge, then their persuasion knowledge is a bigger resource in juding the merits of an agent.
New concepts
"Learn as they go" - Persuasive effects can occur after an advertisment too, or upon repeated viewings. Seeing rival ads will also have this effect.
"Change of meaning" - the moment when the consumer perceives the persuasive techniques of an agent. At first, they will take no particular meaning to actions, but after this pivotal event, they will recognize tactics. The usual outcome is a general detachment and a feeling of the persuastion techniques being off-putting. This is the perception, and happens whether or not the agent actually considers their behavior as a persuasive tactic.
Other theories
PKM can benefit other theories:
Attitude-toward-the-ad research - focuses on the underly assumptions that people use to evaluate ads.
Coaching - coaching aims to increase persuasion knowledge and skills. PKM says they should also acquire "if-then" knowledge, ie, if a certain tactic is used, then what cognitive action they must perform
Elaboration Likelihood Model (ELM) - people are influenced by "peripheral cues" and yes, they are not clear on what peripheral cues are. But PKM can tell them why and how certain types of cues and play signaling roles. Percieved cues may be known as "perceived tactics" in PKM
Heuristic-Systematic Model - people refine topic attitudes learn to conserve cognitive effort by using simple "persuasion heuristics." PKM can identify a tactic is used, for what reason it's used, and assessing an ad's effectiveness. Researchers should also examine things other than the singular goal of refining their topic attitude. For example, heuristic-systematic researchers were once surprised that people saw and ad and drew inferences about the ad makers as well as the product itself. But under PKM, it is expected
Attribution theory accounts of persuasion - focuses on everyday sociocognitive knowledge, and posits general processes in which lay people produce and modify social knowledge structures. So far, the consumer has been depicted as trying to understand why the salesperson or endorser is speaking on behalf of the marketer. In PKM, they will also ask why has the agent chosen this spokesperson, and why has the agent chosen this persuasive technique for the salesperon to use on me?
Future directions
Most research is focused on marketer beliefs and how that affects their ad making. They think about the ad itself, but not how advertisers actually think and how they make their ads persuasive. Another thing that people could research is how people change their minds after the see the advertisment, ie, what happens if you let the consumer think about it overnight?
The ultimate goal is the develop an integrated theory of the interplay between an agent's and a target's persuasion knowledge, that is, what marketers believe and what consumers believe. Two things:
Agents and targets seek to be maxically effective in persuasion production and persuasion coping. Asymmetries may occur.
The validity of persuasion knowledge is difficult to quantify. There are different elements that a person may be good or bad at, but more importantly, it is always relative to the knowledge of the other agent persiasion knowledge. Hmmm.
More work needs to be done on the agent side. Plenty has been done on the consumer.
James Spader likes the control systems engineering equivalent of social cognitive theory!
This is a dynamical systems model of the Social Cognitive Theory. It proven workable with simulations, and when using real data, had a 40% fit with the MILES study.
Definitions
Social Cognitive Theory (SCT)
SCT is one of the most influential theories to guide health behavior interventions.
Habitation
This is a behavioral response, and one of the simplest forms of learning. It consists of spontaneous recovery of a response when the stimulus is withheld, more rapid habituation following prior series of habituation and recovery, and is affected by the effects of requency.
Model
control system dynamic model for SCT
There are 6 vats that can be controlled by flows:
Self-management skills - inputs are behavior
Outcome expectancy - inputs are self-management skills
Self-Efficacy - inputs are self-management skills, feedback loop with behavior
Behavior - inputs are cue to action
Behavioral Outcomes - inputs are behavior
Cue to action - start here, inputs are external and internal cues
Final
When using the MILEs real data, they used:
Input: Skills training (exogenous input 1)
Input: External cues (exogenous input 8)
Output: Self-efficacy (variable 3)
Output: Behavior (variable 1)
The fit between the data and the model output is 49.51% for self-efficacy and 34.95% for behavior. Well, this stuff is hard.
This paper uses a control system to describe time-varying phenomena in a smoking cessation intervention.
Traditionally, interventions are fixed, meaning a simple composition and dosage is given to all participants. In adaptive interventions, the dosage and type of treatment varies according to participant response.
Intensive longitudinal data (ILD) is loosely defined as a quantitative or qualitive data recorded at "more than a handful of time points." Hopefully it is collected more often than that, so that the intervention response can be analyzed with respect to shape, periodicity, and time-dependency.
Structural equation models (SEM) are used to optimize models.
Smoking intervention
4 groups:
AC - buproion and counseling
ANc - buproion and no counseling
PC - placebo and counseling
PNc - placebo and no counseling
Daily evening reports reported:
Urge - urge to smoke
Cigonmind - cigarettes on my mind
Thinksmk - thinking about smoking a lot
Bother - bothered by desire to smoke
Cigsmked - No. of cigarettes smoked
Enthus - enthusiastic
Food - thinking about food a lot
Final
take away message
Final
take away message
James Spader likes applying systems science to behavioral health interventions!
Why not use time-varying "adaptive" interventions? That is, the dosages of the intervention components are assigned based on the assessed values of tailoring variables that refect some outcome measure. They are a closed-loop dynamical system, which puts them in the category of control engineering.
Definitions
Intensive longitudinal data (ILD) is field data that is obtained via ecological momentary assessment (EMA). Data has to be rapidly sampled with continuous time assessments. This is modeled with dynamic modeling and hybrid model predictive control.
Summary
The main goals are:
Optimize inverventions by personalizing treatment through adapatation
Increasing access to ILD through EMA for "closing the loop"
Behavioral theories can help model and control strategy development
Example 1
Fibromyalgia (FM) can be treated with naltrexone.
The time series is split into baseline, placebo, drug, and washout phases. A cursory examination shows a presence of lagged dynamics of naltrexone on other variables.
The modeling process is taken in 3 steps:
The first step is data preprocessing for missing entries.
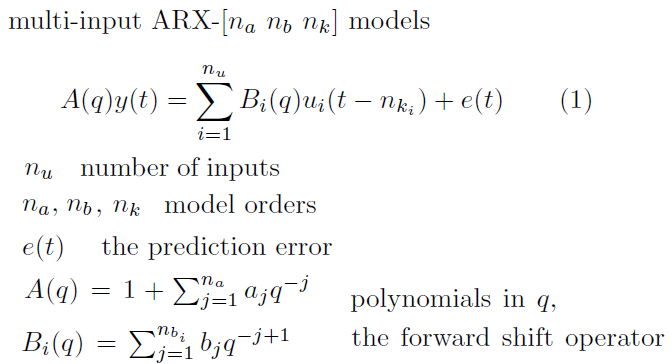
The second step is discrete-time modeling using multi-input ARX models. Watch out for over-parameterization.
Insert variables until you get the highest order needed
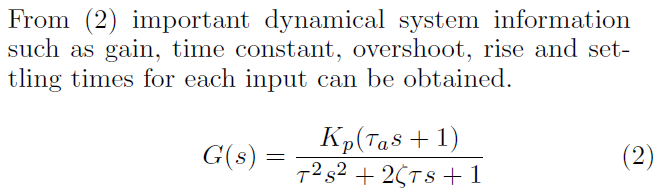
The third step is fitting the responses from the ARX model to this form
The step responses from ARX are invidiually fit to a parisimonious continuous second-order model structure
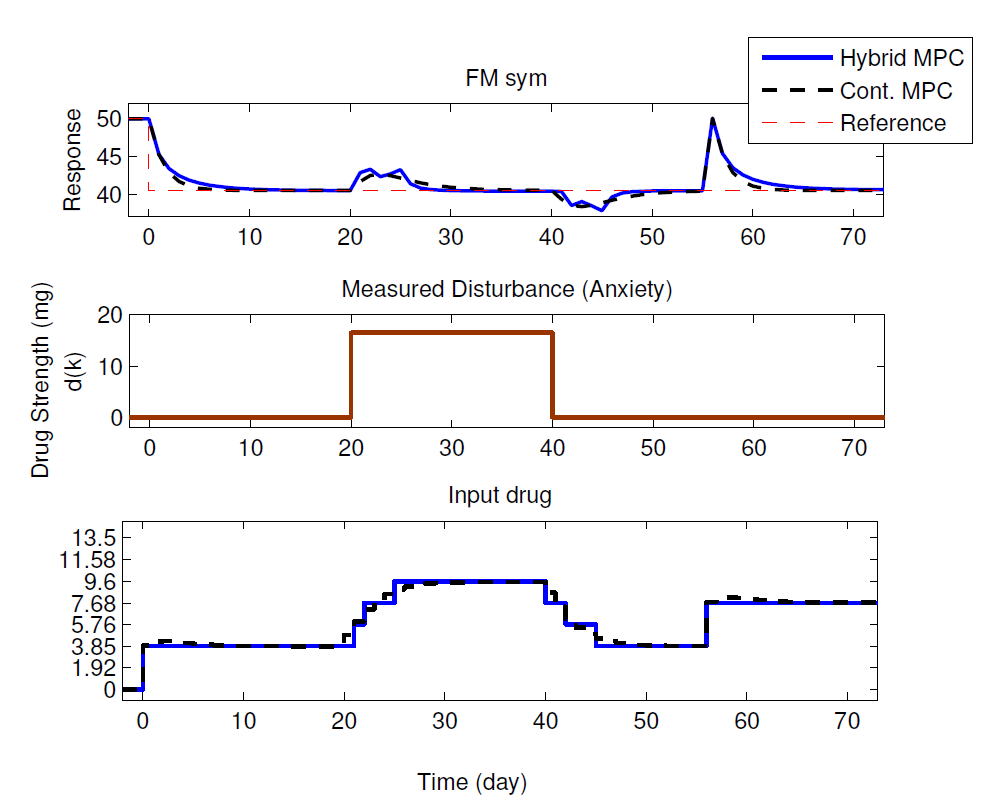
A a hybrid Model Predictive Control (MPC) algorithm performs three functions:
Setpoint tracking -
Measured disturbance rejecting -
Unmeasured distrubance rejection -
Performance of a hybrid MPC (8 levels) compared to a continuous MPC for models from a representative participant.
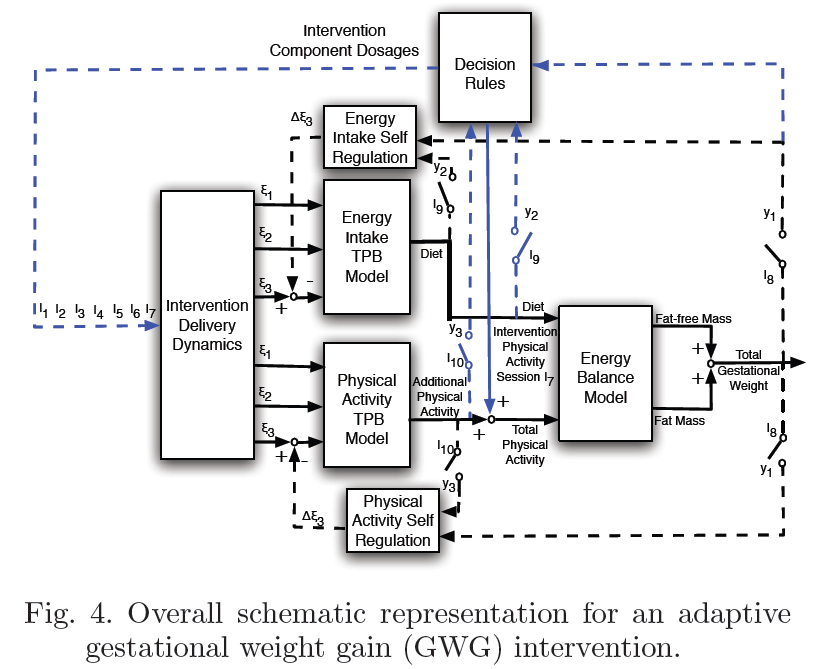
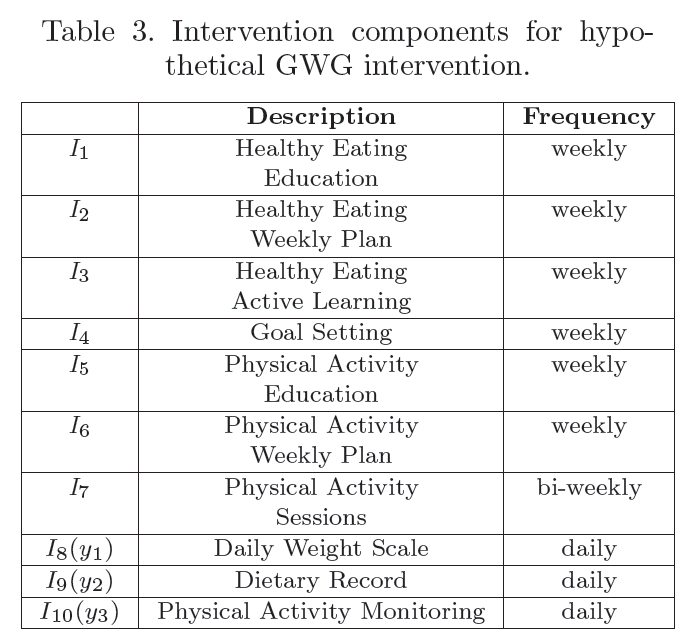
Example 2
Excessive weight gain
schematic
variables in an intervention
take away message
take away message
Final
take away message
James Spader likes a systematic review of mHealth interventions using cell phones!
This is an overview of mobile health interventions that are designed to increase healthy behavior or improve disease management. It als quantifies the effectiveness for mhealth consumers. I am not going to go over all of them, but the relevant categories of interest to me are:
Health behavior change:
smoking cessation
increase physical activity
reduce caloric intake
Disease management:
adherence to medication
Stats
16 Health behavior interventions that used phones. 13/16 used the SMS function.
13/16 used the SMS function
increase physical activity
reduce caloric intake
The maxmimum number of behavioral change techniques was 18, and the media was 6. The most common were:
Feedback on performance: 13 interventions
Goal setting: 12 interventions
Provide information on the consequences of behavior: 11 interventions
Tailoring: 11 interventions
Prompt self-monitoring: 10 interventions
Identify barriers to behavior or identify ways of overcoming barriers: 8 interventions
Takw away message
Smooking cessation: doubled cessation rates at 6 months
Reduce caloric intake: no statistically or clinically significant changes
Increase physical activity: no statistically or clinically significant changes
Diabetes: statistically small effects and borderline clinical importance
Medication adherence: simple reminders show no benefits
What if you got people to record how many sodas they drank a day, weigh themselves on day 7 and 14, and gave them reminders to do so? The reminder was also tailored based on past behavior. If the user drank les soda, it would say, "Well done. You are successfully reducing your fizzy drinks intake." Or if they drank the same amount, it would say, "Your fizzy drinks intake is the same as yesterday."
Results
Average mean soda consumption went from 4.89 sodas per week in week 1, and 2.27 sodas in week 2.
User remarks
Some people do not need reminders: I think reminders were good. For the first two days, I used the reminders. But from the third day, I recorded my fizzu drinks unconsciously.
While others do: I go to the system after receiving the reminders because now I can trust that I am being reminded and I do not need to remember by myself.